|
|
|
|
|
|
1. EUGENICS and PIUS XI (introd.): 1.1. Mendel; 1.2. Darwin; 1.3. Galton; 1.4. US Sterilization; 1.5. Pius XI
3. NÜRNBERG, INFORMED CONSENT, and PIUS XII (introd.): 3.1i. Nurenberg Trials; 3.2. Nurnberg Code; 3.3. Pope Pius XII
4. RESPIRATORS and CPR; 4.1 Chest Compression; 4.2 Respirator; 4.3. Leslie Blackhall on CPR Survival and the Persistent Vegetative State:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. EUGENICS and PIUS XI (introd.) Friedrich Nietzsche Pope Pius XI (p.1922-1939) |
|
|
|
|
|
|
|
|
|
|
|
|
|
1.1.
ABBOT
GREGOR
MENDEL,
(1822-1884)
The Father of Modern Genetics
|
|
|
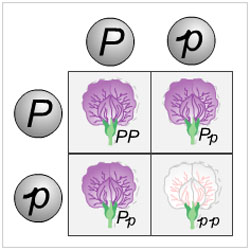
| ABBOT GREGOR MENDEL | Inheritance Patterns in Garden Peas |
|
|
|
| Abbey of St. Thomas, Brno, Czech Republic | Abbey Library |
THE Augustinian Abbot Gregor Mendel published the results of his experiments on garden peas from 1856-1863; but their significance for the developing science of genetics was not appreciated until the turn of the century. The pseudo-science of eugenics attempted to twist Mendel’s science of heredity and fuse it in a muddled way with Friedrich Nietzsche’s notion of a philosophical “superman” (Übermensch) who would evolve beyond the constraints of Christian morality to discover the true potential of human beings.
1.2.
CHARLES
DARWIN
(1809-1882)
Evolution and the Origin of the
Species
|
|
|
|
| CHARLES DARWIN | The Voyage of the Beagle | Darwin in Later Life |
ALTHOUGH Darwin emphasized the necessity for compassion, even when it appears to contradict natural selection, later “Social Darwinists” reinterpreted select passages from the following text:
With savages, the weak in body or mind are soon eliminated; and those that survive commonly exhibit a vigorous state of health. We civilized men, on the other hand, do our utmost to check the process of elimination; we build asylums for the imbecile, the maimed, and the sick; we institute poor-laws; and our medical men exert their utmost skill to save the life of every one up to the last moment. ... Vaccination has preserved thousands who from a weak constitution would formerly have succumbed to smallpox. Thus, the weak members of civilized societies propagate their kind. No one who has attended to the breeding of domestic animals will doubt that this must be highly injurious to the race of man.... Excepting in the case of man himself, hardly anyone is so ignorant as to allow his worst animals to breed.
[Yet,] the aid which we feel impelled to give to the helpless is mainly an incidental result of the [otherwise good] instinct of sympathy.... We must therefore bear the undoubtedly bad effects of the weak surviving and propagating their kind ... (501f)
From Charles Darwin, The Descent of Man (1871)]
1.3.
FRANCIS
GALTON,
(1822-1911)
Founder and Promoter
of The Eugenics Society
|
|
|
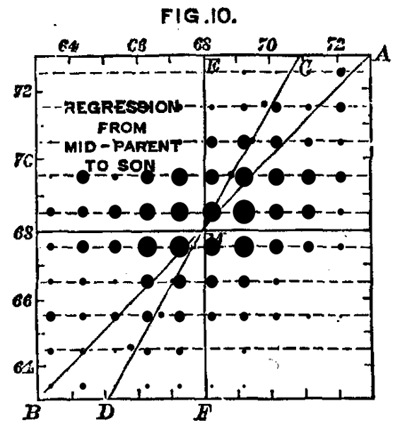
| Sir FRANCIS GALTON | Galton's statistical analysis of inheritance |
|
|
|
|
Galton on the Inheritability of Genius |
Marie Stopes, disciple of Galton: British Champion of Birth Control and lifelong member of the Eugenics Society |
ENGLISH social scientist, [cousin of Darwin, who disapproved of many of Galton's views] made significant contributions to the fields of statistics and heredity, including the first significant twin study in 1883. Described as a virulent racist, he popularized the phrase “nature and nurture” emphasizing the sole importance on intelligence of heredity; he denied the significance of environment on intelligence. [Britannica 98: Galton proposed that a system of arranged marriages between men of distinction and women of wealth would eventually produce a gifted race.] He also coined the term “eugenics” in 1883 and effectively founded the eugenics movement, although his ideas were not widely accepted until the turn of the century and the rediscovery of Mendel's laws of inheritance. Galton founded the Eugenics Society. His ideas were influential on Marie Stopes, an early proponent of contraception in Britain, who had met Galton as a young woman, and who remained a supporter of eugenics and a member of the Eugenics Society throughout her life..
The subject of Race Improvement, or Eugenics, with which I have much occupied myself during the last few years, is a pursuit of no recent interest . . . I think that stern compulsion ought to be exerted to prevent the free propagation of the stock of those who are seriously afflicted by lunacy, feeble- mindedness, habitual criminality, and pauperism, but that is quite different from compulsory marriage. How to restrain ill-omened marriages is a question by itself, whether it should be effected by seclusion, or in other ways yet to be devised that are consistent with a humane and well-informed public opinion. I cannot doubt that our democracy will ultimately refuse consent to that liberty of propagating children which is now allowed to the undesirable classes, but the populace has yet to be taught the true state of these things. A democracy cannot endure unless it be composed of able citizens; therefore it must in self-defence withstand the free introduction of degenerate stock.
From Francis
Galton, Memories of My Life ,
ch, 21, “Race Improvement.”
1.4.
STERILIZATION
LAWS
in the UNITED
STATES
|
|
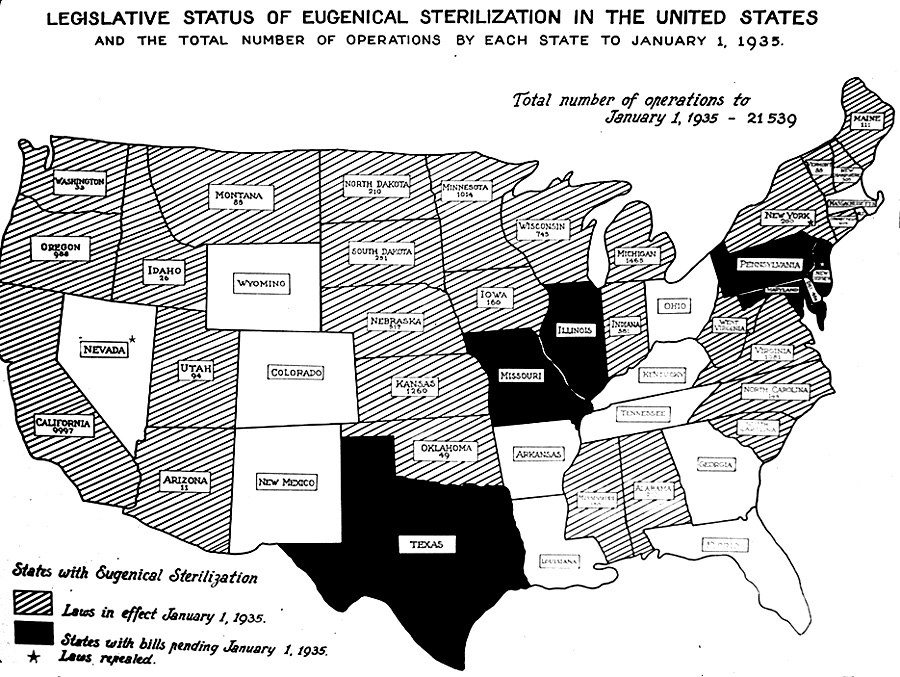
| The Harry H. Laughlin Papers January 1, 1935. Harry Hamilton Laughlin was director of the Eugenics Records Office in Cold Spring Harbor, Long Island, New York from 1910 to 1940 |
Sofair, André N., et.al. “Eugenic Sterilization and a Qualified Nazi Analogy: The United States and Germany, 1930-1945,” Annals of Internal Medicine, 15 Feb. 2000. Vol. 132 no. 4, pp. 312-319
THE history of state-sponsored sterilization in the United States began with legislation in Indiana in 1907. By 1926, 23 states had enacted sterilization laws, which were motivated mainly by eugenic and therapeutic concerns. Eighteen of these states mandated involuntary sterilization of certain mentally defective persons or certain kinds of criminals. In Oregon, Montana, and Idaho, laws provided for both voluntary and involuntary sterilization, and in Iowa, Nebraska, New Hampshire, Minnesota, and Maine, laws provided for voluntary sterilization alone. In all but one of these eight states with voluntary laws (Idaho), consent was not required from a patient if he or she was incapable of giving it; written consent from a relative or guardian was sufficient. Such “voluntary” laws would therefore be more aptly described as nonvoluntary. Most states confined compulsory sterilization to inmates of public mental institutions, in which the proportion of poor and minority residents was greater than that in the general population; for instance, inmates sterilized in Virginia and California were disproportionately black or foreign-born, respectively.
California and eight other states were responsible for most of the eugenic sterilizations performed under state laws.
The cumulative number of sterilizations in these states by 1943 was
16,553 in California,
4472 in Virginia
2706 in Kansas
2388 in Michigan
2111 in Minnesota
1597 in Oregon
1372 in Wisconsin
1346 in North Carolina
1231 in Indiana
By 1944, 30 states with sterilization laws had reported a total of more than 40,000 eugenic sterilizations; of those sterilized,
20,600 were reported as insane and
20,453 as feebleminded.
In the pre-Nazi period, German eugenicists expressed admiration for U.S. leadership in instituting sterilization programs and communicated with their U.S. colleagues about strategies .
Despite waning scientific and public support and the history of the human rights abuses of Nazi Germany, state-sponsored sterilizations in the United States continued long after the war, totaling approximately 22000 in 27 states between 1943 and 1963.
André N. Sofair, MD, MPH; and Lauris C. Kaldjian, MD. "Eugenic Sterilization and a Qualified Nazi Analogy: The United States and Germany, 1930-1945". Annals of Internal Medicine 15 February 2000 Volume 132 N. 4, pp. 312-319.
May 2, 1927 - Justice Oliver Wendell
Holmes
The case of Buck v. Bell decided on this day is a now-notorious Supreme Court decision upholding the constitutionality of a compulsory sterilization law in Virginia. Justice Oliver Wendell Holmes, in explaining his decision, famously –or infamously– said “three generations of idiots is enough.”
Carrie Buck was an 18-year-old confined in the Virginia State Colony for Epileptics and Feebleminded. The superintendent said she had the mental age of a 9-year-old (although evidence now disputes that judgment). The Supreme Court upheld the constitutionality of the sterilization order, 8–1, with Justice Oliver Wendell Holmes writing the Court’s opinion.
Justice Oliver Wendell Holmes for the
[Supreme]Court:
(1927, Buck vs. Bell, Superintendent of State Colony
Epileptics and Feeble Minded)
“We have seen more than once that the public welfare may call upon the best citizens for their lives. It would be strange if it could not call upon those who already sap the strength of the State for these lesser sacrifices, often not felt to be such by those concerned, in order to prevent our being swamped with incompetence. It is better for all the world if, instead of waiting to execute degenerate offspring for crime or to let them starve for their imbecility, society can prevent those who are manifestly unfit from continuing their kind. . . . Three generations of imbeciles are enough.”
In the 1920s, the idea of eugenics was broadly supported by the medical and scientific communities. Partly as a result of Nazi policies in Germany, however, thinking about developing a “pure” race changed radically, and the Buck decision is now generally reviled by civil libertarians and human rights activists. See the case of Skinner v. Oklahoma, decided on June 1, 1942, in which the Supreme Court declared unconstitutional an Oklahoma law requiring the sterilization of certain criminal offenders.
1.5.
THE
RESPONSE
of the CATHOLIC
CHURCH
to EUGENICS:
POPE
PIUS
XI
on CHRISTIAN
MARRIAGE
|
|
CASTI
CONNUBII
Encyclical of Pope Pius XI Pope Pius XI (1922-1939) |
|
|
|
|
68. FINALLY, that pernicious practice must be condemned which closely touches upon the natural right of man to enter matrimony but affects also in a real way the welfare of the offspring. For there are some who over solicitous for the cause of eugenics, not only give salutary counsel for more certainly procuring the strength and health of the future child - which, indeed, is not contrary to right reason - |
Reprobetur denique oportet perniciosus ille usus, qui proxime quidem naturale hominis ius ad matrimonium ineundum spectat, sed ad prolis quoque bonum vera quadam ratione pertinet. Sunt enim qui, de finibus eugenicis nimium solliciti, non solum salubria quaedam dent consilia ad futurae prolis valetudinem ac robur tutius procurandum — quod rectae rationi utique contrarium non est — |
|
but put eugenics before aims of a higher order, and by public authority wish to prevent from marrying all those whom, even though naturally fit for marriage, they consider, according to the norms and conjectures of their investigations, would, through hereditary transmission, bring forth defective offspring. |
sed cuilibet alii etiam altioris ordinis fini eugenicum anteponant, et coniugio auctoritate publica prohiberi velint eos omnes ex quibus, secundum disciplinae suae normas et coniecturas, propter hereditariam transmissionem, mancam vitiosamque prolem generatum iri censent, etiamsi iidem sint ad matrimonium ineundum per se apti. |
|
And more, they wish to legislate to deprive these of that natural faculty by medical action despite their unwillingness; and this they do not propose as an infliction of grave punishment under the authority of the state for a crime committed, not to prevent future crimes by guilty persons, |
Quin immo naturali illa facultate, ex lege, eos, vel invitos, medicorum opera privari volunt; neque id ad cruentam sceleris commissi poenam publica auctoritate repetendam, vel ad futura eorum crimina praecavenda, licebit, |
|
but against every right and good they wish the civil authority to arrogate to itself a power over a faculty which it never had and can never legitimately possess. |
scilicet contra omne ius et fas ea magistratibus civilibus arrogata facultate, quam numquam habuerunt nec legitime habere possunt. |
|
|
|
|
69. Those who act in this way are at fault in losing sight of the fact that the family is more sacred than the State and that men are begotten not for the earth and for time, but for Heaven and eternity. Although often these individuals are to be dissuaded from entering into matrimony, certainly it is wrong to brand men with the stigma of crime because they contract marriage, on the ground that, despite the fact that they are in every respect capable of matrimony, they will give birth only to defective children, even though they use all care and diligence. |
Quicumque ita agunt, perperam dant oblivioni sanctiorem esse familiam Statu, hominesque in primis non terrae et tempori, sed caelo et aeternitati generari. Et fas profecto non est homines, matrimonii ceteroqui capaces, quos, adhibita etiam omni cura et diligentia, nonni si mancam genituros esse prolem conicitur, ob eam causam gravi culpa onerare si coniugium contrahant, quamquam saepe matrimonium iis dissuadendum est. |
|
|
|
| 70. Public magistrates have no direct power over the bodies of their subjects; therefore, where no crime has taken place and there is no cause present for grave punishment, they can never directly harm, or tamper with the integrity of the body, either for the reasons of eugenics or for any other reason. | Publici vero magistratus in subditorum membra directam potestatem habent nullam; ipsam igitur corporis integritatem, ubi nulla intercesserit culpa nullaque adsit eruentae poenae causa, directo laedere et attingere nec eugenicis nec ullis aliis de causis possunt unquam. |
|
St. Thomas teaches this when inquiring whether human judges for the sake of preventing future evils can inflict punishment, he admits that the power indeed exists as regards certain other forms of evil, but justly and properly denies it as regards the maiming of the body. “No one who is guiltless may be punished by a human tribunal either by flogging to death, or mutilation, or by beating.”[Summ. theol., 2a 2ae, q. 108 a 4 ad 2um.] |
Idem docet Sanctus Thomas Aquinas, cum, inquirens num humani iudices ad futura mala praecavenda hominem possint malo quodam plectere, id quidem concedit quod ad quaedam alia mala, sed iure meritoque negat quod ad corporis laesionem «Numquam secundum humanum iudicium aliquis debet puniri, sine culpa, poena flagelli, ut occidatur, vel mutiletur vel verberetur» (56). |
|
|
|
|
71. Furthermore, Christian doctrine establishes, and the light of human reason makes it most clear, that private individuals have no other power over the members of their bodies than that which pertains to their natural ends; and they are not free to destroy or mutilate their members, or in any other way render themselves unfit for their natural functions, except when no other provision can be made for the good of the whole body. |
Ceterum, quod ipsi privati homines in sui corporis membra dominatum alium non habeant quam qui ad eorum naturales fines pertineat, nec possint ea destruere aut mutilare aut alia via ad naturales funetiones se ineptos reddere, nisi quando bono totius corporis aliter provideri nequeat, id christiana doctrina statuit atque ex ipso humanae rationis lumine omnino constat. |
|
|
|
|
|
|
|
|
|
|
|
|
|
2.
ANTIMICROBIALS; |
|
|
|
|
|
|
|
|
|
|
2.1. ANTIBIOTICS: SULFA DRUGS Sulfanilamides
|
|
|
| PAUL DOMAGK | Prontosil |
Gerhard Johannes Paul
DOMAGK
(1895-1964), a biochemist working for the Bayer Corporation in Germany,
discovered that azo dyes like prontosil were effective against streptococcal
infections in mice. He and others were unconvinced that these
compounds would work in humans, because they do not prevent bacterial growth by
themselves. As it turns out, these drugs ARE
effective because they are bacteriostatic: i.e. they inhibit growth of
organisms, relying on the body’s immune reaction to dispose of the bacteria that
can no longer divide.
In 1932 his daughter cut her hand, contracted a severe infection, and was near death. In desperation, Domagk gave her a dose of prontosil, and she made a rapid and complete. He kept this secret until the clinical studies were over and he had published his findings in 1935. Domagk was awarded the Nobel Prize but the Nazi government refused to let him accept it.
2.2. ANTIBIOTICS: PENICILLIN
|
|
|
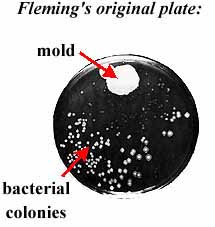
| ALEXANDER FLEMING | Fleming's Petrie Dish |
PENICILLIN. Although discovered by Alexander Fleming in 1928, who observed inhibition of strep colonies by mold, initial attempts to purify penicillin in Oxford in early 1940s were not commercially successful. It was not purified in sufficient quantity to be useful until 1942 (Pfizer, USA)
In 1929 Alexander Fleming (1888-1955) England, described how a mould, Penicillium had destroyed [bacterial colonies on a petrie dish]. He did little work with the discovery but it was realized that this could be an approach to destroying bacteria. In 1939 Howard Florey and Ernst Chain at Oxford produced pure Penicillin from the mold and in 1940 they "cured" 4 streptococcus- infected mice while 4 controls died. They then tried penicillin on humans, testing it on a policeman who was dying of Staphylococcal septicemia - he responded but they ran out of penicillin, despite recycling it from his urine, and he died. The great value of such a drug was recognized, but wartime Britain did not have the resources to produce it. So that in 1941 Penicillin was given to the USA for production. Penicillin was found to be highly effective against Staphylococcus and Streptococcus
(adapted from P. Warren, The Medical Treatment of Disease, lecture: http://www.umanitoba.ca/faculties/medicine/units/history/notes/treatment/)
2.3. INTRAVENOUS THERAPY
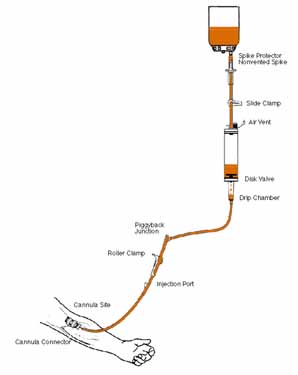 |
INTRAVENOUS THERAPY Used successfully during a cholera epidemic in 1832 by two physicians, Thomas Latta and Robert Lewins, but not seriously attempted again for 60 years (until the 1890s). Usefulness still debated during WW I. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.
NÜRNBERG,
INFORMED
CONSENT, Trial of Fritz Ter Meer Pope Pius XII |
|
|
|
|
|
|
|
|
|
|
|
|
|
THE doctrine of informed consent, as it is interpreted today in the United States and most western nations, underwent significant evolution throughout the second half of the twentieth century. The "doctor trials" at Nürnberg disabused a horrified world of all naïveté concerning the extent to which the medical profession can always be trusted. Nürnberg demanded that informed and free consent must always and forever be obtained from subjects in medical experiments. But by the nineteen-seventies the application of this principle broadened considerably, and in the United States it came to encompass all non-emergency medical procedures. To put it bluntly, in the United States today any non-emergent medical treatment performed without the patient's consent may constitute a crime that can be prosecuted, not merely as medical malpractice, but as assault.
|
|
|
| The Nürnberg Trials | Herman Goehring |
3.1.
INTRODUCTION
The Proof as to War Crimes and Crimes against Humanity
Judged by any standard of proof the record clearly shows the commission of war crimes and crimes against humanity substantially as alleged in counts two and three of the indictment. Beginning with the outbreak of World War II criminal medical experiments on non-German nationals, both prisoners of war and civilians, including Jews and “asocial” persons, were carried out on a large scale in Germany and the occupied countries.
|
|
|
|
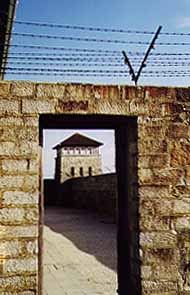
| Mauthausen | Nazi freezing experiments | Mauthausen |
These experiments were not the isolated and casual acts of individual doctors and scientists working solely on their own responsibility, but were the product of coordinated policy-making and planning at high governmental, military, and Nazi Party levels, conducted as an integral part of the total war effort. They were ordered, sanctioned, permitted, or approved by persons in positions of authority who under all principles of law were under the duty to know about these things and to take steps to terminate or prevent them.
Permissible Medical Experiments
The great weight of evidence before us is to the effect that certain types of medical experiments on human beings, when kept within reasonably welldefined bounds, conform to the ethics of the medical profession generally. The protagonists of the practice of human experimentation justify their views on the basis that such experiments yield results for the good of society that are unprocurable by other methods or means of study. All agree, however, that certain basic principles must be observed in order to satisfy moral, ethical and legal concepts.
3.2.
The Ten Principles of the
NÜRNBERG CODE
1. The voluntary consent of the human subject is absolutely essential.
This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment.
The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.
2. The experiment should be such as to yield fruitful results for the good of society, unprocurable by other methods or means of study, and not random and unnecessary in nature.
3. The experiment should be so designed and based on the results of animal experimentation and a knowledge of the natural history of the disease or other problem under study that the anticipated results will justify the performance of the experiment.
4. The experiment should be so conducted as to avoid all unnecessary physical and mental suffering and injury.
5. No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.
6. The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
7. Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability, or death.
8. The experiment should be conducted only by scientifically qualified persons. The highest degree of skill and care should be required through all stages of the experiment of those who conduct or engage in the experiment.
9. During the course of the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible.
10. During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject [....]
|
|
3.3. MEDICAL
EXPERIMENTS |
An address given September 13 (or 14?), 1952 by Pope Pius XII to the First International Congress on the Histopathology of the Nervous System.
12. In the first
place it must be assumed that, as a private person,
the doctor can take no measure or try no course of action
without the consent of the patient.
The doctor has no other rights or power over the patient than those which the
latter gives him, explicitly or implicitly and tacitly. On his side, the patient
cannot confer rights he does not possess. In this discussion the decisive point
is the moral licitness of the right a patient has to dispose of himself. Here is
the moral limit to the doctor’s action
taken with the consent of the patient.
13. As for the patient, he is not absolute master of himself, of his body or of his soul. He cannot, therefore, freely dispose of himself as he pleases. Even the reason for which he acts is of itself neither sufficient nor determining. The patient is bound to the immanent teleology laid down by nature. He has the right of use, limited by natural finality, of the faculties and powers of his human nature. Because he is a user and not a proprietor, he does not have unlimited power to destroy or mutilate his body and its functions. Nevertheless, by virtue of the principle of totality, by virtue of his right to use the services of his organism as a whole, the patient can allow individual parts to be destroyed or mutilated when and to the extent necessary for the good of his being as a whole. He may do so to ensure his being’s existence and to avoid or, naturally, to repair serious and lasting damage which cannot otherwise be avoided or repaired.
14.
The patient, then, has no right
to involve his physical or psychic integrity in
medical experiments or research
when they entail serious
destruction, mutilation, wounds or perils.
|
|
|
|
|
|
|
|
|
|
4.
CARDIO
-
PULMONARY
RESUSCITATION 1937 “iron lung” |
|
|
|
|
|
|
|
|
|
|
4.1. CARDIO -
PULMONARY
RESUSCITATION (CPR)
MOUTH-to-MOUTH
RESUSCITATION
HIST: http://www.lifesaving.com/issues/articles/10evolution.html
Ancient methods of resuscitation included:
1. the application of heat, excrement or ashes;
2. flagellation
|
|
|
|
More recent methods include:
16th century: blowing hot air and smoke into the victim's lungs with a bellows
|
|
|
|
|
18th century:
1. instilling smoke into the rectum;
2. “inversion” (hanging drowning victims
upside-down);
3. rolling victims over a barrel.
4. placing victim on trotting horse.
19th century:
1. rolling victims 16 times per minute from
side-to-back,
applying pressure to the back
while prone;
2. stretching the tongue
Modern CPR developed in the late 1950s and early 1960s. Dr. James O. Elam (1954) demonstrated the superiority of expired air ventilation without equipment over manual chest pressure; his work was confirmed during the next four years by Dr. Peter Safar. The American Red Cross mounted a campaign to teach mouth-to-mouth resuscitation for drowning victims.
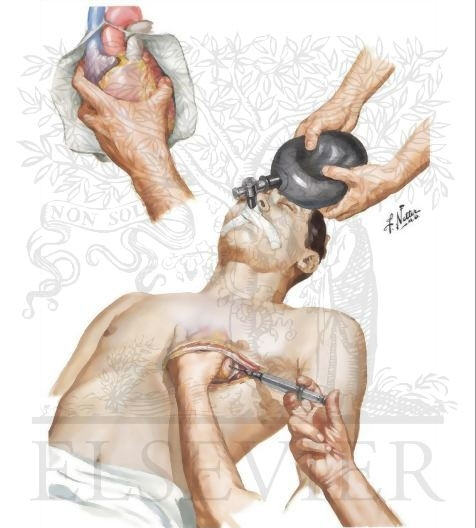
CHEST
COMPRESSIONS
FROM 1950-1960 direct cardiac compression by squeezing the heart by hand through a hole cut in the left side of the victim's chest. The success rate was very low.
|
|
|
| internal cardiac massage | External Chest Compression |
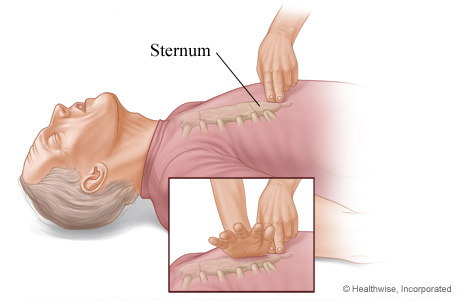
In early 1960 Drs. Kouwenhoven, Knickerbocker, and Jude discovered the benefit of chest compression to achieve a small amount of artifical circulation. Later in 1960, mouth-to-mouth and chest compression were combined to create CPR as it is practiced today.
|
|
| Locate and avoid the Xyphoid Process |
4.2.
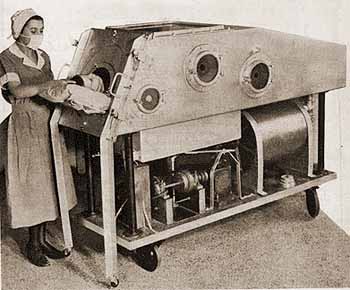
RESPIRATORS
IN 1928, Philip Drinker and Louis Shaw at Harvard Medical School introduced the “iron lung” to help individuals suffering from acute poliomyelitis.
|
|
|
Polio impaired patients' ability to breathe by paralyzing the diaphragm and intercostal muscles; the iron lung provided relief in the form of artificial respiration.
|
|
|
 |
|
| 1955 Infant “iron lung” | Child in “iron lung” | Paul Alexander †78, 2024 | Modern Respirator |
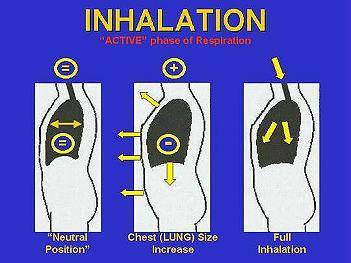
IT consisted of a sealed chamber in which air pressure is alternately reduced and increased. The patient was placed in the chamber with his/her head emerging from a port at one end. Each cycle of vacuum within the chamber allowed their lungs to be filled with atmospheric air; subsequent increase of pressure forced exhalation of air from the lungs.
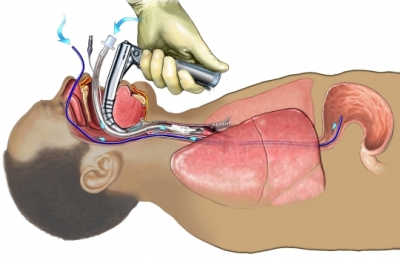
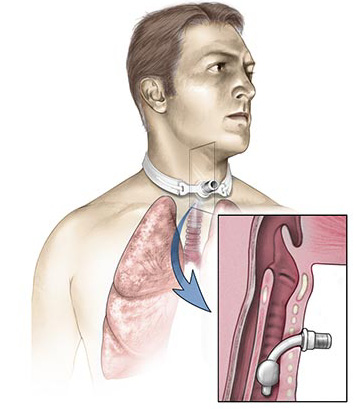
MODERN respirators provide “positive-pressure breathing” through a tube placed down the trachea
|
|
|
or inserted through a hole in the neck, leading into the trachea.
|
|
 |
|
CARDIOVERSION
|
|
4.3.
MUST
WE
ALWAYS
USE
CPR?
Leslie J. Blackhall,
M.D.
New England Journal of Medicine,
“Sounding Board”
Nov. 12, 1987; vol. 317, No. 20, pp. 1281-1285. Webpage;
MS-Word
Doc
PDF Doc
It is clear that survival after CPR is related to the underlying illness that leads to the arrest and that patients with certain conditions very rarely survive. For example, Bedell et al., in a study of 294 consecutive patients who had cardiac arrest at the Beth Israel Hospital in Boston, found that although 44 percent initially responded to CPR, only 14 per-cent survived until discharge.
No patient with metastatic cancer survived until discharge, nor did any patient with
an acute stroke
sepsis, or
pneumonia.
Only 2 percent of patients with severe cardiomyopathy
and 2 percent of patients who had had hypotension for 24 hours survived.
Only 3 percent of the patients with renal failure (defined as a blood urea nitrogen level >50 mg per deciliter) survived, and
no patient who required dialysis or had oliguria for 24 hours before the cardiac arrest survived until discharge. [...]
In all these papers, we see a discrepancy between the initial response rate (16 to 45 percent) and survival until discharge (5 to 23 percent overall, with less than 5 percent survival in many groups). Studies that considered the length of survival of patients who were initially resuscitated but died before discharge found that these patients lived an average of 2 to 14 days, usually in an intensive care unit. The risk of the development of a chronic vegetative state after CPR was 2 percent in the paper by Johnson et al. and 2.7 percent in a paper by Messert and Quaglieri (10 percent of the patients who survived CPR in their study). Thus, although the number of patients who are in a chronic vegetative state after CPR is small, in many disease categories, it approaches the number who survive CPR. [...]
CPR is a desperate technique that works relatively infrequently, and in many types of patients, virtually never. To solve the ethical dilemmas posed by CPR we must first face that medical fact. Furthermore, as we have seen, there is potential harm in CPR in that patients may be kept alive for days to weeks undergoing painful and dehumanizing procedures with no conceivable medical benefits. Because of these facts, we need to reevaluate the ways we use CPR. Too often CPR just happens, without inquiry into the patient’s wishes or consideration of its chances of success. Both patient autonomy and physician responsibility are important factors in making decisions regarding CPR. In cases in which CPR has any potential for success, the principle of patient autonomy dictates the patient’s right to choose or refuse such treatment. In order for patients to exercise this right, however, two conditions must be met. First, patients need to be given sufficient information concerning the likely outcome of CPR and the risks involved, so that an informed decision can be made. Second, because CPR is attempted unless patients have been asked whether they wish it and have refused it, physicians need to involve their patients earlier and more frequently in the decision to use CPR.
Note that the statistics on survival to discharge after in-hospital CPR have not changed significantly since the publication of this article in 1986, .i.e. 12-15%:
[1] “Cardiopulmonary resuscitation in intensive care unit and non-intensive care unit patients. Immediate and long-term survival.” Karetzky. M., Arch Intern Med, June 26 1995; 155(12), 1277-80.
[2] “Efficacy of CPR in a general, adult ICU,” Myrianthefs P., Resuscitation, April, 2003; 57(1):43-8.
[3] “Epidemiologic Study of In-Hospital Cardiopulmonary Resuscitation in the Elderly”, Ehlenbach, W., N Engl J Med., July 2, 2009; 361:22-31.
[4] “Survival after in-hospital cardiopulmonary resuscitation,” Saghafinia, et al. Saudi J Anaesth Vol. 4, Issue 2, May-August 2010 68-71
[5] “Predictors of survival after cardiac or respiratory arrest in critical care units,” Kutsogiannis, et al. Canadian Medical Association Journal, October 4, 2011, 183(14) 1589-1595
[5] “Survival after in-hospital cardiopulmonary resuscitation from 2003 to 2013, An observational study before legislation on the life-sustaining treatment decision-making act of Korean patients,” Young, et al., Medicine 99(30), July 24, 2020. [12%]
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002