|
|
|
|
|
|
|
|
CYSTIC HYGROMA and FETAL HYDROPS |
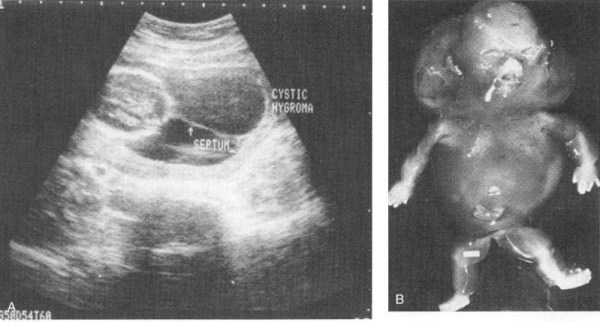
Definition: the term “hygroma” means moist tumor. Cystic hygromas are anomalies of the lymphatic system characterized by single or multiple cysts within the soft tissues, usually involving the neck.
Incidence: Cystic hygroma’s were found in 1 in 200 spontaneously aborted fetuses with crown-rump length greater than 3 cm.
Explanation: A congenital malformation resulting from the so called jugular lymphatic obstruction sequence, and is due to a lack of communication between the cervical lymphatic vessels and the jugular venous system. This is a lethal anomaly that has long been recognized in aborted fetuses, often associated with generalized hydrops. However, if a communication between the two systems occurs before fetal death, the hygroma may regress leaving redundant skin folds in the neck(pterygium colli).
The majority of female fetuses with cystic hygroma probably have Turner’s syndrome. This, the ultrasound detection of a cystic pouch at the back of the neck is highly suggested of monosmy x. However, nuchal hygromas are also part of other malformation syndromes, such trisomy 21, Noona’s syndrome and Robert’s syndrome. In addtion, a few familair observations of cystic hygromas suggest that this condition may also be inherited as an autosomal recessive trait.
Associated Anomalies: Cystic hygromas are very frequently associated with chromosomal aberrations and, consequently, with a wide variety of anatomic defects.
Hydrops: edema. Retaining of fluids in the body. Hydrops and generalized edema are more frequently associated with cystic hygromas.
Marked edema or fetal hydrops, results from vascular damage and high output heart failure.
Prognosis: The prognosis is different depending on the presence or absence of associated hydrops. In our experience, the mortality rate of cystic hygromas with fetal hydrops is 100%. Prognosis data about fetal cystic hygromas without associated hydrops are scanty.
The natural history of fetal cystic hygromas has not been clearly extablished. Some infants diagnosed in the second trimester with isolated hygromas may develop nonimmune hydrops as gestation progesses. Others may undergo canalization of the lymphatic channels and resolution of the hygromas. Regression results in redundant skin in the cervical region and webbed neck.
FETAL HYDROPS |
Definition: Hydrops fetalis (fetal hydrops) is a serious condition caused by Rh sensitization and other conditions. A fetus affected by hydrops becomes extremely swollen because of buildup of fluid in the body tissues. Organs such as the liver and spleen become enlarged, the fetus develops anemia, and the ability of the fetus’s blood to carry oxygen is decreased.
Even with treatment, fetal hydrops can cause death of the fetus.
Links
associated with Cystic Hygroma
Please submit any websites that address the topics of Cystic Hygroma,
Fetal Hydrops or associated disorders.
Contact A Family - Contact Group started in 1983. It offers contact with other parents where possible. It publishes a periodic newsletter. The group represents around 200 families in the UK, mainly with affected children. Additionally the group has contact with families in Australia and the USA.
BabyCenter.com Forum regarding Cystic Hygroma
|
|
|
|
SUPORTIVE WEBSITES |
http://www.cystichygroma.co.uk/
Wednesday 07/13/2005 5:03:38pm
Name: kath mullen
E-Mail: kamullen_123@yahoo.com
Location:
liverpool U.K.
Comments:
i am currently 24
weeks pregnant and have had numerous tests as my consultant thought my baby had
severe chromosome abnormalities at 11 weeks. I had an amnio done and was told
everything is fine, I have since gone onto scans to check the organs and heart
for abnormatilies - they haven't found anything wrong. In passing my consultant
said that the baby has a cystic hygroma of 11mm on the back of her head. She
didn't seem concerned and said it may go away - Ive gone onto various web sites
looking for info and now worried at what ive found. Is there anyone out there in
the same situation with any advice? I would be most grateful
x
Friday 07/08/2005 7:32:54am
Name: Celena Roldan
E-Mail: celena_roldan@yahoo.com
Just Surfed In
Location:
San Pedro, California
Comments:
Hi everyone,
My name is Celena I am now 21. At 9 mo. I was diagnosed with Cystic Hygroma. I
have minor affects from the seven surgeries that took place between the age of 9
mo. and 6 yrs old. The left side of my face droops from nerve damage. I am left
with the usage of one side of my lung and one vocal cord.
For the first year after my surgeries I was unable to produce sound, they didn't
think I would be able to ever talk. Through high school I was a cheerleader, so
much for not being able to produce sound. Still today my voice is very low and
raspy. It is frustrating sometimes to be in noisy environments, where I am
unable to be heard. I know I should be grateful for my ability to speak, but I
can’t help wanting to have the full capacity of my voice.
I am very insecure about my appearance and my voice. I have had cosmetic surgery
to compensate for the nerve damage. It's been fifteen years since my last
encounter with cystic hygroma, hopefully that means it is gone for good! This
site has been very uplifting to know that there are others out there. Please
email me or write me I would like to share experiences. I am graduating from
SDSU this year, woo hoo!!!!
~Celena
2910 Alma St.
San Pedro, Ca 90731
celena_roldan@yahoo.com
Tuesday 01/25/2005 6:23:32pm
Name:
Sallietta M. Bedford
E-Mail:
Homepage Title:
csbrinson
Homepage URL:
Referred By:
Search Engine
Location:
Lady Lake Florida
Comments:
Son was born with a
hygroma the size of a grape fruit at birth. Removed at six weeks old. Had
plastic surgery. Nerves were damaged. Required G- Tube.
Lost hearing in right ear. Nerves healed G tube out. Eyes, smile is perfect.
Cytoxin medication was administered in the 80's. The past 3 years he has had a
few problems with the hygroma reoccuring. The hygromas are pressing on his
airway causing breathing difficulty. Emergency Tracheoscopy in December 2004. If
all goes well it should be temporary. Cbrinson is 21 years old. Born 03/21/1983.
Christopher is trying to recuperate so that he may continue his education in the
Music Production. Any friends in this area Orlando, Lake County area.
PATHOLOGY
of NON-IMMUNE
HYDROPS
|
Nonimmune Hydrops
The three major causes of nonimmune hydrops include
cardiovascular defects, chromosomal anomalies, and fetal anemia (see Table 10-5
).[60] Both structural and functional cardiovascular defects, such as congenital
cardiac defects and arrhythmias, may result in intrauterine cardiac failure and
hydrops. Among the chromosomal anomalies, 45,X karyotype (Turner syndrome) and
the trisomies 21 and 18 are associated with fetal hydrops. Most often,
underlying structural cardiac anomalies associated with the chromosomal
aberrations form the basis of fetal hydrops. In the Turner phenotype, however,
abnormalities of lymphatic drainage from the neck may lead to postnuchal fluid
accumulation (cystic hygromas). Fetal anemia, not caused by Rh- or ABO-associated
antibodies, also results in hydrops. In fact, in some parts of the world (e.g.,
Southeast Asia), severe fetal anemia due to homozygous α-thalassemia is probably
the most common cause of nonimmune hydrops.[61] Transplacental infection by
parvovirus B19 is rapidly emerging as an important cause of hydrops. The virus
gains entry into erythroid precursors (normoblasts), where it replicates,
leading to erythrocyte maturation arrest and aplastic anemia. Parvoviral
intranuclear inclusions can be seen within circulating and marrow erythroid
precursors (see Fig. 10-9 ). The basis for hydrops in fetal anemia of both
immune and nonimmune etiology is tissue ischemia with secondary myocardial
dysfunction and circulatory failure. Additionally, secondary liver failure may
ensue, with loss of synthetic function contributing to hypoalbuminemia, reduced
oncotic pressure, and edema. Approximately 10% of cases of nonimmune hydrops are
related to monozygous twin pregnancies and twin-to-twin transfusion occurring
through anastomoses between the two circulations.
Morphology of Hydrops Fetalis.
The anatomic findings in fetuses with intrauterine fluid accumulation vary with both the severity of the disease and the underlying etiology. As previously noted, hydrops fetalis represents the most severe and generalized manifestation, and lesser degrees of edema such as isolated pleural, peritoneal, or postnuchal fluid collections can occur. Accordingly, infants may be still-born, die within the first few days, or recover completely. The presence of dysmorphic features suggests the presence of a constitutional chromosomal abnormality; postmortem examination may reveal an underlying cardiac anomaly. In hydrops associated with fetal anemia, both fetus and placenta are characteristically pale; in most cases the liver and spleen are enlarged from cardiac failure and congestion. Additionally, the bone marrow demonstrates compensatory hyperplasia of erythroid precursors (parvovirus-associated aplastic anemia being a notable exception), and extramedullary hematopoiesis is present in the liver, spleen, and possibly other tissues such as the kidneys, lungs, and even the heart. The increased hematopoietic activity accounts for the presence in the peripheral circulation of large numbers of immature red cells, including reticulocytes, normoblasts, and erythroblasts (erythroblastosis fetalis)