|
|
|
|
|
|
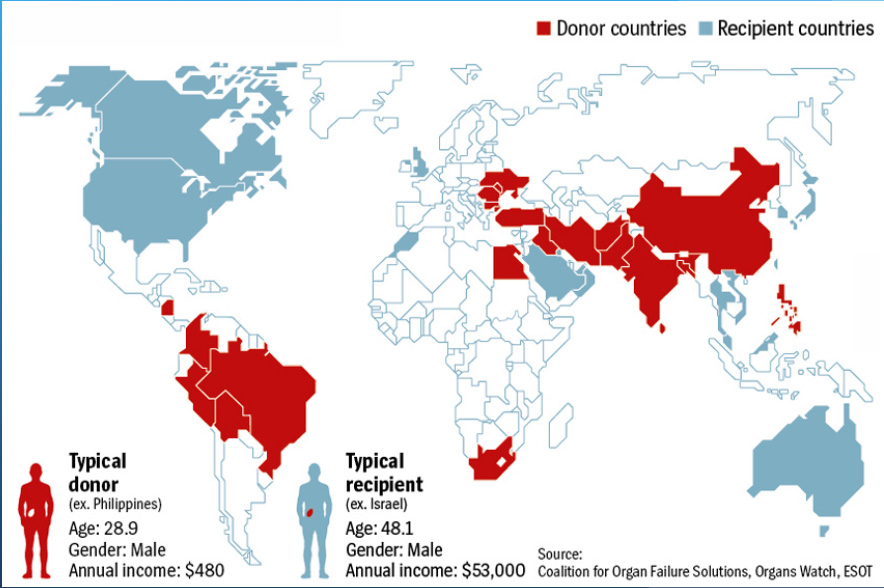
IN every country of the world except Iran it is illegal to financially entice prospective donors to donating their organs. Altruism on the part of the donor: namely, genuine concern for the afflicted recipient, is almost universally regarded as the only legitimate motive for live-organ donation. Nevertheless, the secretive world of organ “trafficking” is an indisputable reality, and has become a world-wide source of exploitation of the poor and disadvantaged.
Parts
unknown: Undercover ethnography of the organs-trafficking
underworld
Nancy Scheper-Hughes
Ethnography 2004; 5; 29
DOI: 10.1177/1466138104041588
PARTS-UNKNOWN.PDF PARTS UNKNOWN-DOC
Α militant anthropology beyond bioethics
In the Anthropology of Reason (1996), Rabinow characterized one dominant mode of social science practice, the vigilant virtuoso, which he exemplified in the work of Pierre Bourdieu, whose guardian spirit hovered over the Ethnografeast. The defining moment for Bourdieu’s reflexive sociology was the unveiling of the lie – the illusion – of those forms of collective and individual self-deception necessary to maintain any social group: a marriage; a family; a profession; a community; or a society. The power of the sociological-anthropological imagination derives from the social scientist’s claim to occupy a privileged position outside the social field and the powerful interests at play within it. Achieving such extraordinary clarity of vision demands a sacrifice – the refusal of all social action and the rejection of all personal interest in the meaning and stakes of social life. Rabinow characterized this stance as based on a set of ascetic techniques, central to which is a renunciation of the ‘real’ world – the world of power, action and high stakes.
But Bourdieu had long embraced what he himself called the life of an ‘engaged and militant intellectual’. In one of his last public lectures delivered in Athens in May 2001, Bourdieu discussed his active, sometimes combative, engagement with social movements, labor unions, the homeless, displaced rural workers, against the worldwide embrace of economic and cultural globalization that he insisted was a dangerous theory of social reality rather than a description of it. In his public lecture ‘Unite and Rule’, Bourdieu referred to the ‘global market’ as a political creation, and to globalization as a psuedo-concept masking a kind of neo-evolutionary model of the world in which a city or a nation’s insertions into the global market (where cities are classified as ‘global’, for example) are diagnostic of a new kind of developmental trajectory. Given the gravity of the world situation, Bourdieu called for the practice of ‘a scholarship with commitment’ toward building collective structures capable of giving birth to new social movements and new sites for international action.
It is in that same spirit that I am arguing here for a dual vision of anthropology as a disciplinary field, a traditional field of study, and as a force field, a site of political struggle and resistance. Another aspect of the struggle is epistemological. As Laura Nader has often pointed out, the truly radical promise of our discipline lies in its ability to question taken-for-granted assumptions and to problematize the received and conventional wisdoms of the day by virtue of our insistence upon reading the world from a topsy-turvy and outsider view of institutions and power relations.
Transplant surgeons often see themselves as embattled by overly cautious social norms that stand in the way of their ability to save or to prolong the lives of their patients. Most would rather not have to consider where the organs they need come from or just how they were obtained. The procurement of organs (both legal and illicit) is generally managed by third (and supposedly neutral and less self-interested) parties. Meanwhile, surgeons tend to be pragmatic thinkers who individualize ethical dilemmas and are often oblivious to the ‘larger picture’, such as the effects and consequences of certain biomedical practices and procedures on the well-being of society (the social body) or on the health of the political body, the body politic.
Transplant stories are generally told from the patient-recipient’s point of view and in a deeply affecting, emotional, rhetorical, even ideological language of gift-giving, altruism, reciprocity, lifesaving and heroism. To this day, transplant surgeries still evoke biblical sentiments and images of resurrection and of doctor-healers ‘raising the dead’.16 Thus, like visionary shamans, transplant surgeons wear a mantle of charisma that protects (sometimes even exempts) their work from critical scrutiny, especially from outside the ranks of the profession.17 Nor are bioethicists, who are so closely identified with medicine and its projects, able to break ranks with powerful biomedical and biotechnological interests. They are too embedded within the medical culture on which they are attempting to comment. ‘Morality’, writes the philosopher of selfless love, Emmanuel Levinas, ‘does not belong to culture; it enables one to judge it’ (1988: 100).
Anthropologists, archetypal ‘professional strangers’ and traveling people, are better positioned to examine social and medical values from an unaligned, inside–outsider perspective and to bring into the equation the ‘view from afar’ as well as people, places and things that are often hidden from view.
There is a growing consensus today among the international transplant community and among the world’s leading bioethicists that paid organs procured from living donors will soon supplant cadaveric donation for those organs. The sale of organs from living humans is, at least for the time being, limited to one kidney, half of a liver, or one lung – in other words those organs that are divisable or that exist ‘in duplicate’. Thus, surgical practices that, not so long ago, were viewed as almost unthinkable violations of medical ethics have over a short period of time and in some parts of the world become almost routine despite the fact they still constitute violations of national laws and international regulations that prohibit and/or condemn the buying and selling of human body parts.
Today, ethical debates in transplant medicine no longer concern the redefinition of life, death and brain death (see Lock, 2000, 2002) but rather the conditions – altruistic, compensated, or some blend of gift, sale, theft and barter – under which organs may be procured from living donors. Today the lines are drawn between those who support some form of regulated sales (Friedlander, 2002; Radcliffe-Richards et al., 1998) and those who argue for continued ‘prohibition’ (see Delmonico and Scheper-Hughes, 2002) and for a renewed commitment to increase the availability of cadaver organs by various means including financial ‘incentives’ (see Delmonico et al., 2002), or by imposing national systems of ‘presumed consent’ (in its most radical form, redefining the dead body as communal or state property), through xenotransplant (the use of animal, mainly pig, organs which is becoming a realistic possibility), and through human stem cell research and experimentation with genetically altered organs.
What is going by the wayside in these new illicit medical transactions are not only laws and long-standing medical regulations but the very bedrock supporting traditional medical ethics – modernist and humanist conceptions of bodily holism, integrity and human dignity. It might be fair to ask if ‘the life’ that is teased out of the body of the one and transferred into the body of the other bears any resemblance to the ethical life of the free citizen (bios) or whether it more closely resembles the bare or naked life of the slave. Here, I am referring to the distinction made by Giorgio Agamben (1998), drawing on Aristotle’s Politics, between bios, the proper life of the citizen, and zoe – the mere, brute life of the species. Thomas Aquinas would later translate these ancient Greek concepts into medieval Christian terms distinguishing the natural life from the good life.18
But neither Aristotle nor Aquinas are with us. Instead, we are asked to take counsel from the new discipline of bioethics which has been finely calibrated to meet the needs of advanced biomedical procedures/biotechnologies and the desires of postmodern medical consumers.19 Even as conservative a scholar as Francis Fukuyama refers to the ‘community of bioethicists’ as having ‘grown up in tandem with the biotech industry ... and [at times] nothing more than sophisticated (and sophistic) justifiers of whatever it is the scientific community wants to do’ (2002: 204).
Not surprisingly, bioethics has offered little resistance to the growing markets in humans and body parts. Today the ‘right’ to buy or sell human organs is increasingly defended in the world’s premier medical journals, including The Lancet and JAMA, among others. Recently, a highly respected transplant professional defended the patient’s ‘right to buy’ an organ as a ‘mellowing’ and ‘maturing’ of medical ethics (Friedlaender, 2002). This maturation process to which he refers is the attempt to thoroughly rationalize transplant medicine, stripping it of its early religious trappings (see below) and of its humanist biases so as to bring it into alignment with neoliberal conceptions of the human, the body, labor, value, rights and economics.
In effect, the corrective field of bioethics and the profession of transplant medicine have both capitulated to the dominant market ethos. Growing numbers of transplant doctors now argue that the real problem lies with outdated laws, increasingly irrelevant national regulatory agencies (like UNOS) and archaic medical professional norms that are out of touch with transplant realities today and with the ‘quiet revolution’ of those who have refused to face a premature death with equanimity and ‘dignity’ while waiting patiently on an official waiting list for a cadaver organ. Some argue for a free trade in human organs; others argue for a regulated market.
Transplant surgeons sometimes see themselves as ‘above the law’. The younger generation of transplant doctors sees themselves as societal mavericks breaking down ‘old taboos’ standing in the way of advancing technological capabilities. In the face of illicit transplants with paid donors, a great many kidney transplant surgeons simply look the other away. Some actively facilitate an informal sale that will save or improve the life of one of their patients. Others prepare and counsel kidney patients for transplant trips overseas and admire the initiative of those who have returned having purchased a kidney from a hapless women in a Lima slum or from an executed Chinese prisoner, as the case may be. Patient autonomy, individual freedom, the right to choose and the commitment to a utilitarian ethos of ‘the greatest good for the greatest number’ guide the sense of ‘the ethical’ in these illicit transplant practices.
In the rational choice language of contemporary medical ethics the conflict between non-malfeasance (‘do no harm’) and beneficence (the moral duty to perform good acts) is increasingly resolved in favor of the libertarian and consumer-oriented principle that those able to broker or buy a human organ should not be prevented from doing so. Paying for a kidney ‘donation’ is viewed as a potential ‘win-win’ situation that can benefit both parties (see Radcliffe-Richards et al., 1998). Individual decision making and patient autonomy have become the final arbiters of medical and bioethical values. Social justice and notions of the ‘good society’ hardly figure at all in their discussions.
Continuing to articulate the current dilemma of transplant, under these new social conditions, in terms of scarcity, supply and demand – when the precious ‘commodities’ in question are increasingly attached to living bodies – creates serious ethical dilemmas for the patients and for their doctors who find themselves in the position of passively and inadvertently, or actively, creating a medically protected space for the kidney commerce. ‘Who am I to second guess, let alone to judge, my patients?’, Michael Friedlaender, a kidney transplant specialist at Hadassah Hospital, asked me with reference to the growing numbers of patients in his hospital-based practice who have returned from overseas having purchased a kidney.
Later, he was to write:
Here began my conversion from fierce objection to kidney marketing to passive acquiescence in this trade. We could not prevent our patients travelling to Iraq [later to Turkey, Romania, and the US]. We gave patients who asked our advice all the information I have presented here, and warned them that we could not help them outside our national boundaries, but assured them that we would immediately assist them on their return. (Friedlaender, 2002: 971–2)
‘If my own kidneys failed I would opt for a transplant from a living donor’, Dr Friedlaender has said on more than one public occasion. The data on different survival rates are circulated widely among kidney transplant surgeons around the world, and are frequently cited by their patients and directly contribute to the decision to abandon conventional cadaver organ waiting lists in pursuit of ‘fresh’ kidneys from living people.
Another consumer-based stimulus behind the occult economy in living donor kidneys and part-livers (see Liver4you@yahoo.com) is the growing rejection of hemodialysis by increasingly sophisticated kidney patients. Dialysis treatment for any period of time, even as a bridge while waiting for transplant, is increasingly viewed by kidney activists as unacceptable suffering, as time on the cross. In September 2000 a young man I will call Amatai, a 23-year-old university student from Jerusalem, flew to New York City for a kidney transplant with an organ purchased from a local ‘donor’ arranged through a broker in Brooklyn. Most of the cost of the surgery (US$200,000) was paid for by his Israeli ‘sick funds’ (medical insurance that is guaranteed to all Israeli citizens). Particularly noteworthy in his narrative was the almost seamless naturalization of living donation and the rejection of the artificiality of the dialysis machine:
Kidney transplant from a living person is the most natural solution because you are free of the [dialysis] machine. With transplant you don’t have to go to the hospital three times a week to waste your time for three or four hours. And after each dialysis you don’t feel very well, and you sleep a lot, and on weekends you feel too tired to go out with your friends . . . Look, dialysis isn’t a normal life. You are limited to certain foods. You are not allowed to eat a lot of meat, salt, fruits, vegetables. Even if you are careful, sometimes your skin becomes yellow. Aesthetically, dialysis isn’t very nice. A kidney transplant from a living donor is the very best solution.
At the same time, many kidney patients resist the idea of conventional ‘waiting lists’ for cadaver organs as archaic vestiges or residues of wartime triage and rationing, or worse, as reminiscent of socialist bread lines and petrol ‘queues’. In the present climate of biotechnological optimism and biomedical triumphalism, the very idea of a shortage, even an organs shortage, suggests a basic management, market or policy failure. The ideology of the global economy is one of unlimited and freely circulating goods. And those new commodities are evaluated, like any other, in terms of their quality, durability and market value.
In the late modern consumer-oriented context, the ancient prescriptions for virtue in suffering and grace in dying can only appear patently absurd. But the transformation of a person into a ‘life’ that must be prolonged or saved at any cost has made life into the ultimate commodity fetish. And an insistence on the absolute value of a single human life saved, enhanced or prolonged ends all ethical or moral inquiry and erases any possibility of a global social ethic. Meanwhile, the traffic in kidneys reduces the human content of all the lives it touches.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002
