|
|
|
|
|
|
In the practice of organ donation after cardiac death the organ donor is not brain dead. It is possible when patients (or their surrogate decision-makers) have decided to have life support withdrawn, and who wish also to donate organs after their death. Life support is withdrawn in an operating room, and after the heart has stopped beating for a specified period, organs are removed for transplantation. As will be seen, this raises various concerns and even conflicts: the team caring for the patient wishes to provide all appropriate palliative care; while the transplant team wishes to preserve the organs in as usable a state as possible. These two approaches entail vary different procedures and techniques.
1.
ORGAN
DONATION
AFTER
CARDIAC
DEATH
Robert Steinbrook, M.D.
N Engl J Med 2007;
357:209-213. July 19, 2007
ALTHOUGH the numbers of organ donors and transplantations in the United States have more than doubled over the past 20 years (see line graph.), the demand for organs continues to dwarf the supply. In 2006, there were about 29,000 solid-organ transplantations; as of June 2007, there were about 97,000 people on waiting lists for organ transplantation.
![]()
Organ Donors and Transplantations in the United States, 1988–2006
About three of every four organs that are transplanted are recovered from deceased donors. The most rapid increase in the rate of organ recovery from deceased persons has occurred in the category of donation after “cardiac death” — that is, a death declared on the basis of cardiopulmonary criteria (irreversible cessation of circulatory and respiratory function) rather than the neurologic criteria used to declare “brain death” (irreversible loss of all functions of the entire brain, including the brain stem). Organs were recovered from 645 donors after cardiac death in 2006, as compared with 189 in 2002; these donors accounted for 8% of all deceased donors in 2006 (see bar graph
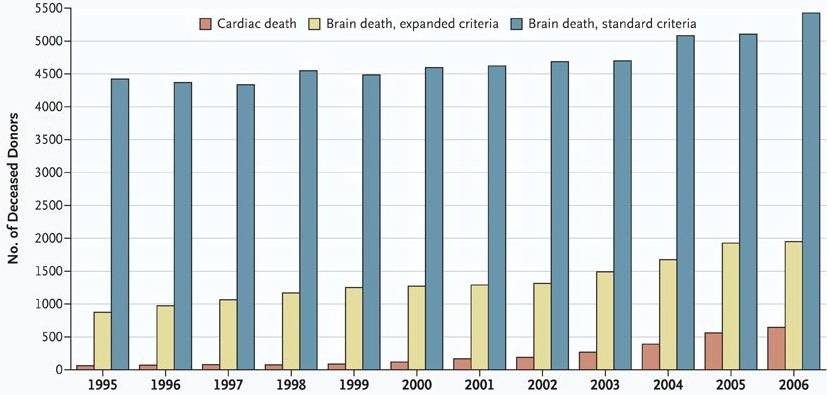
Distribution of Deceased Organ Donors in the United States, 1995–2006
At the Organ Procurement Organization at the University of Wisconsin, the New England Organ Bank in the Boston area, and the Finger Lakes Donor Recovery Network in New York, such donors accounted for more than 20% of all deceased donors.
Since 1968, when an ad hoc committee at Harvard Medical School proposed a brain-based definition of death that became widely accepted, organs for transplantation have been removed primarily from hospitalized patients who have been pronounced dead on the basis of neurologic criteria, when they are on ventilators and their hearts continue to function. The continued circulation of blood helps to prevent the organs from deteriorating.
Obtaining organs from donors after cardiac death — when the heart is no longer beating — is the approach that was generally followed in the 1960s and earlier. Today, such donations typically involve patients who are on a ventilator as the result of devastating and irreversible brain injuries, such as those caused by trauma or intracranial bleeding. Potential donors might also have high spinal cord injuries or end-stage musculoskeletal disease. Although such patients may be so near death that further treatment is futile, they are not dead.
The United Network for Organ Sharing, a private nonprofit group based in Richmond, Virginia, operates the Organ Procurement and Transplantation Network under contract with the federal government and is committed to increasing the number of donors. OPTN/UNOS, as the networks are collectively known, has developed rules for donation after cardiac death. According to these rules, finalized in March 2007, the process begins with the selection of a suitable candidate and the consent of the legal next of kin to the withdrawal of care and retrieval of organs. Subsequently, life-sustaining measures are withdrawn under controlled circumstances in the intensive care unit (ICU) or the operating room; donation after an unexpected fatal cardiac arrest is rare.
When the potential donor meets the criteria for cardiac death, a doctor pronounces the patient dead. The time from the onset of asystole — the absence of sufficient cardiac activity to generate a pulse or blood flow (not necessarily the absence of all electrocardiographic activity) — to the declaration of death is generally about 5 minutes, but it may be as short as 2 minutes.1 The limited data available suggest that circulation does not spontaneously return after it has stopped for 2 minutes.2 The organs — most commonly the kidneys and liver but also the pancreas, lungs, and, in rare cases, the heart — are then recovered. To avoid obvious conflicts of interest, neither the surgeon who recovers the organs nor any other personnel involved in transplantation can participate in end-of-life care or the declaration of death.
The outcomes for organs transplanted after cardiac death are similar to those for organs transplanted after brain death. However, the length of time varies as to which organs can be deprived of oxygen (the interval from cessation of circulation to the initiation of perfusion with cold preservation solutions) and still be transplanted successfully. It is best to retrieve the liver less than 30 minutes after the withdrawal of life-sustaining measures; the kidneys and pancreas may often be recovered up to 60 minutes after such withdrawal.1 The extent of a patient’s remaining circulatory and respiratory function may reveal whether death is likely to follow soon after extubation. If a patient does not die quickly enough to permit the recovery of organs, end-of-life care continues and any planned donation is canceled. At present, this may happen in up to 20% of cases.
In 1997, 2000, and 2005, the Institute of Medicine reviewed and voiced support for donation after cardiac death.3 In 2005, a conference on donation after cardiac death concluded that it is “an ethically acceptable practice of end-of-life care, capable of increasing the number of deceased-donor organs available for transplantation.”1 Nonetheless, some physicians and nurses at the bedside “continue to have concerns about the ethical propriety of the practice” that “are numerous, complex and related to the specific roles they play.”4 Some feel uncomfortable about participation in medical practices that may be required during the transition from end-of-life care to organ donation.5 For example, in multidisciplinary ICUs, doctors and nurses who care for both potential organ donors and organ recipients may have conflicting interests. They may be uncomfortable recommending the withdrawal of life-sustaining treatment for one patient and hoping to obtain an organ for another.
According to the “dead donor rule,” donation should not cause or hasten death.3 As currently practiced, donation after cardiac death inevitably raises more concerns than donation after brain death. The process is more complex, and the potential donor is not dead when life-sustaining measures cease. The intervals between withdrawing care, pronouncing death, and recovering organs are very brief, and the family’s relation to the dying process may be affected. In an interview, Sue McDiarmid, a professor of pediatrics and surgery at the University of California, Los Angeles, and the immediate past president of OPTN/UNOS, said, “The perception of some physicians and families is that the end-of-life experience is changed because organ procurement begins immediately after death has occurred. However, many families find great solace in the ability to donate organs under these special circumstances.”
Concerns were raised by a February 2006 case in San Luis Obispo, California, that was publicized earlier this year by the Los Angeles Times. Two transplant surgeons were allegedly in the same room with a potential donor, and one of the surgeons allegedly ordered massive doses of morphine and lorazepam in an attempt to hasten the patient’s death and thereby obtain his organs more quickly. The patient did not die for several hours, and his organs were not recovered because they were no longer usable for transplantation. The case, which has been investigated by local law-enforcement authorities, is a sobering reminder that organ-donation efforts can go terribly wrong if appropriate procedures are not followed.
Typically, potential donors are wheeled to the operating room when they are still alive. With explicit consent, heparin — possibly along with other agents — is administered to maintain organ function. According to the 2005 Institute of Medicine conference, providing heparin at the time of withdrawal of life-sustaining treatment “is the current standard of care” because “the long-term survival of the transplanted organ may be at risk if thrombi impede circulation to the organ after reperfusion.”1 Theoretically, heparin could hasten death by causing bleeding, but there is no evidence that it does so in practice. Some protocols also call for the advance placement of catheters in large arteries and veins to facilitate the rapid infusion of organ-preservation solutions after death.1
In January 2007, the Joint Commission (formerly the Joint Commission on Accreditation of Healthcare Organizations) implemented its first accreditation standard for donation after cardiac death. According to this standard, hospitals with the necessary resources must develop donation policies in conjunction with their medical staff and their organ-procurement organization that address “opportunities for asystolic recovery” of organs. Since many hospitals have never had an organ donor whose death was declared on the basis of cardiopulmonary criteria, meeting the standard may require new approaches to both organ donation and end-of-life care. The standard, however, requires that relevant hospitals have the policies in place, not that they allow the practice — they can choose to opt out because of concerns about ethics, quality of end-of-life care, or other reasons. When a hospital and its medical staff decide not to provide for donation after cardiac death and the organ-procurement organization is not in accord, the hospital must document its efforts to reach an agreement and include in the donation policy its justification for opting out. In addition, as of July 1, 2007, OPTN/UNOS has required all 257 transplant hospitals and 58 organ-procurement organizations in the United States to comply with its new rules.
If the number of organ donations after cardiac death continues to increase, more patients will be able to receive transplants. At present, however, these donations remain troubling to some and are not as widely accepted as donations after brain death.4,5 Broader experience with the recommended practices should help, but concerns are likely to persist.
All organ-procurement organizations and transplant centers in the United States must develop and comply with protocols to facilitate the recovery of organs from donors after cardiac death, according to the Organ Procurement and Transplantation Network and the United Network for Organ Sharing (known collectively as OPTN/UNOS). Listed here are “model elements” that the protocols are required to address, as adopted by the OPTN/UNOS board of directors in March 2007; they became effective on July 1, 2007.
“A patient . . . who has a non-recoverable and irreversible neurological injury resulting in ventilator dependency but not fulfilling brain death criteria may be a suitable candidate for donation after cardiac death. Other conditions [may] include end stage musculoskeletal disease, pulmonary disease, and high spinal cord injury.”
“The decision to withdraw life-sustaining measures must be made by the hospital’s patient care team and legal next of kin, and documented in the patient chart.” Depending on the circumstances, the “legal next of kin” may be a relative, a designated health care representative, or an appropriate surrogate.
The assessment of potential donors “should be conducted in collaboration with the local organ procurement organization and the patient’s primary health care team.” The medical director of the organ-procurement organization and transplant-center teams may be consulted.
“An assessment should be made as to whether death is likely to occur (after the withdrawal of life-sustaining measures) within a time frame that allows for organ donation.”
The legal next of kin may consent to the administration of drugs, such as heparin, or procedures, such as the placement of femoral catheters, for the purposes of organ donation. “No donor related medications shall be administered or donation related procedures performed without consent.”
Clearance from the medical examiner or coroner “must be obtained when applicable.” There should be plans for continued end-of-life care and immediate notification of the family “if death does not occur within the established timeframe after the withdrawal of life-sustaining measures.”
“A surgical timeout is recommended prior to the initiation of the withdrawal of life-sustaining measures.” The intent is to verify patient identification and the roles and responsibilities of the various personnel.
“No member of the transplant team shall be present for the withdrawal of life-sustaining measures,” such as removal of an endotracheal tube or termination of medications for blood-pressure support. “No member of the organ recovery team or organ procurement organization staff may participate in the guidance or administration of palliative care, or the declaration of death.”
If applicable, placement of femoral catheters and the administration of heparin or other pharmacologic agents “for the sole purpose of donor organ function must be detailed in the consent process.”
“The patient care team member that is authorized to declare death must not be a member of the organ procurement organization or organ recovery transplant team. The method of declaring cardiac death must comply in all respects with the legal definition of death by an irreversible cessation of circulatory and respiratory function before the pronouncement of death.”
“Following the declaration of death by the hospital care team, the organ recovery may be initiated.”
“Organ procurement organization policy shall be to ensure that no donation related charges are passed to the donor family.”
1 Bernat JL, D’Alessandro AM, Port FK, et al. Report of a national conference on donation after cardiac death. Am J Transplant 2006;6:281-291
2 DeVita MA. The death watch: certifying death using cardiac criteria. Prog Transplant 2001;2:58-66
3 Institute of Medicine. Organ donation: opportunities for action. Washington, DC: National Academies Press, 2006.
4 DuBois JM, DeVita M. Donation after cardiac death in the United States: how to move forward. Crit Care Med 2006;34:3045-3047
5 Mandell MS, Zamudio S, Seem D, et al. National evaluation of healthcare provider attitudes toward organ donation after cardiac death. Crit Care Med 2006;34:2952-2958
2. THE
BOUNDARIES
of ORGAN
DONATION
AFTER
CARDIAC
DEATH
Robert Steinbrook, M.D.
N Engl J Med 2007;
357:209-213. July 19, 2007
Organ donation after circulatory (or cardiac) death has become an accepted medical practice over the past 15 years.1 Programs permitting such donations satisfy two needs: they provide organs in addition to those procured after brain death, and they fulfill the wish of family members that relatives with severe brain injuries serve as organ donors after cessation of life-sustaining therapy and subsequent death. The proliferation of protocols for donation after circulatory death has been spurred by the publication of three reports by the Institute of Medicine (IOM), support by the Department of Health and Human Services, and the establishment of criteria for such donation by the Joint Commission, which accredits U.S. hospitals. A 2005 national conference on the topic identified areas of consensus in an effort to standardize practice.2
Now that donation after circulatory death has become mainstream, researchers have begun to design innovative protocols that aim to improve the function of transplants and expand the donor pool. These protocols test the conceptual limits of donation after circulatory death — by permitting invasive intervention in living organ donors or by altering the tests required to determine death. In this issue of the Journal, Boucek et al. (pages 709–714) report their success with a research protocol for the donation of infant hearts after circulatory death, in which they shortened the duration of asystole required for the determination of death to less than that in prevailing standards of practice. To determine whether such protocols should be incorporated into standards of practice, we must analyze them within the context of accepted principles of organ transplantation from deceased donors and test them against the conceptual basis for death determination.
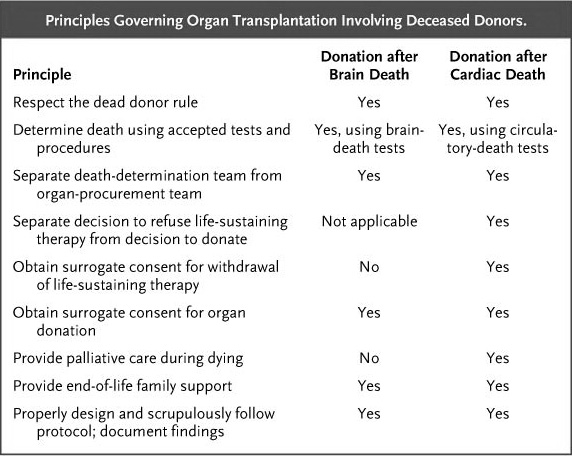
Principles Governing Organ Transplantation Involving Deceased Donors.
The decision of a patient (or a surrogate) to have life-sustaining therapy withheld should precede and remain independent of the decision to donate organs. The strict separation of these two decisions ensures that society’s need or a physician’s request for organs does not drive the decision to withdraw treatment — a possibility that may be even more of a concern when the patient and potential organ donor is a child.3 In most cases, the inherent conflict may be mitigated (but not eliminated) by having a representative from the local organ-procurement organization, rather than physicians in the intensive care unit (ICU), speak to families about donation.
The physician team determining death must be strictly separated from the procurement team to prevent organ-procurement considerations from influencing the death determination. This separation of roles is even more critical in donation after circulatory death than in donation after brain death, because the former requires the withdrawal of life-sustaining therapy, which should be done by the donor’s ICU physician. The recent allegations against Dr. Hootan Roozrokh in San Luis Obispo, California, demonstrates the serious problems that may result from the conflict created when a transplantation surgeon manages the terminal care of a potential organ donor.
The process of withdrawing life-sustaining therapy and providing appropriate palliative care for a dying patient should be the same, irrespective of the patient’s donor status. The situation becomes complicated, however, when a protocol permits intervention in the living donor through the administration of intravenous heparin or vasodilators, not to benefit the donor patient but only to improve the function of transplantable organs. Protocols instituting extracorporeal membrane oxygenation (ECMO) in the donor after the declaration of death permit much more invasive intervention, including the insertion of arterial catheters before death. Advocates assert that surrogate consent sufficiently justifies these interventions, because they are minimally harmful to the patient and they benefit the organ recipient. Opponents argue that respect for the dying patient is being compromised.
The dead donor rule states that the donor must be dead before vital organs are procured. Death statutes require the irreversible cessation of circulation and respiration or the irreversible cessation of brain functions; the former constitutes an adequate criterion for death because, in the absence of cardiopulmonary resuscitation (CPR) or autoresuscitation, it inevitably leads to the fulfillment of the brain criterion.4
What duration of asystole proves irreversibility? The IOM has recommended that after the withdrawal of life-sustaining therapy, physicians wait 5 minutes after the onset of asystole to be certain that a heart rhythm sufficient to generate a pulse does not resume spontaneously. In such circumstances, autoresuscitation has never been reported after 65 seconds of asystole. Physicians can confidently declare the donor dead after 5 minutes of asystole and apnea, because without autoresuscitation or CPR, the cessation of circulatory and respiratory functions is permanent (will not return), and it inevitably and rapidly becomes irreversible (cannot return).4
In their investigational protocol, Boucek et al. shortened the interval of required asystole to 75 seconds on the grounds that 60 seconds was the longest reported duration of asystole that had been followed by autoresuscitation and that the sooner death can be declared after asystole, the less damage from warm ischemia will occur in the organs. What minimum duration of asystole ensures that autoresuscitation will not occur is an empirical question that can be answered conclusively only after observing many hundreds of patients. The recommended duration of asystole required for donation after circulatory death should be determined by scientific and public policy considerations. The IOM and the Canadian Council for Donation and Transplantation purposely chose a conservative duration of 5 minutes, which has been adopted by most donation programs, but a few protocols use as short a span as 2 minutes. In 2005, participants in a national conference on donation after circulatory death agreed with the recommendation by the Society of Critical Care Medicine to wait at least 2 minutes and at most 5 minutes.2
An unanswered question is whether cardiac transplantation from a donor declared dead according to a circulatory criterion retroactively negates the determination of death. Does the fact that a donor’s heart is restarted in another patient prove that circulatory cessation was not irreversible? Or should the requirement of irreversibility be restricted to circulation within the donor?
Another unconventional protocol used by several hospitals for donation after circulatory death involves providing ECMO to the donor immediately after death is declared. If ECMO adequately provided circulation and oxygenation to the donor’s entire body, it would retroactively negate the death determination by preventing the loss of circulation and respiration from becoming permanent or irreversible, potentially “reanimating” the heart and preventing the progression to brain destruction on which the circulatory criterion of death is predicated.
A University of Michigan ECMO protocol for procuring abdominal organs apparently avoids this problem.5 During ECMO, an intraaortic occlusion balloon blocks all blood flow above the diaphragm so that only the abdominal organs are perfused with oxygenated blood. The thoracic organs and brain are isolated from this perfusion circuit and are destroyed by ischemic infarction. If blood flow above the diaphragm is successfully blocked, this protocol does not negate the previous determination of death. Ex vivo ECMO, in which the procured organ is temporarily perfused and preserved after removal from the donor’s body, is another technique that is under investigation.
These investigational protocols test the permissible societal boundaries of donation after circulatory death. To what extent should society permit manipulation of an organ donor or alteration of the determination of human death for the good of organ recipients? A consensus-driven oversight process should determine whether investigational protocols reflect appropriate medical treatment and whether their translation into accepted clinical practice is sound public policy. Leaders of the critical care, neurology, and transplantation communities need to jointly draft practice guidelines for organ donation after circulatory death that establish acceptable boundaries of practice. These boundaries should be based on scientific data and accepted principles and should be demarcated conservatively to maintain public confidence in the integrity of the transplantation enterprise. I predict that when prudent boundaries are created, they will exclude whole-body ECMO of the donor and death determinations at 75 seconds of asystole.
1 Steinbrook R. Organ donation after cardiac death. N Engl J Med 2007;357:209-213
2 Bernat JL, D’Alessandro AM, Port FK, et al. Report of a national conference on donation after cardiac death. Am J Transplant 2006;6:281-291
3 Mandell MS, Zamudio S, Seem D, et al. National evaluation of healthcare provider attitudes toward organ donation after cardiac death. Crit Care Med 2006;34:2952-2958
4 Bernat JL. Are organ donors after cardiac death really dead? J Clin Ethics 2006;17:122-132
5 Magliocca JF, Magee JC, Rowe SA, et al. Extracorporeal support for organ donation after cardiac death effectively expands the donor pool. J Trauma 2005;58:1095-1102
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002