|
|
Faust: Wagner creates the homunculus. |
|
|
Faust: Wagner creates the homunculus. |
1. BIOLOGY and TECHNOLOGY of In Vitro Fertilization
2. THE MAGISTERIUM on IVF: 2.1 Donum Vitae; 2.2. Dignitas Personae; 2.3. Humanae Vitae; 2.4. Theology of the Body; 2.5. Evangelium Vitae
3. COMPLICATIONS and SIDE-EFFECTS of IVF; 3.1. Ovarian Hyperstimulation; 3.2. Birth Defects; 3.3 Multiple Gestations
1. BIOLOGY
and TECHNOLOGY
of In Vitro Fertilization
As Ford has noted (The Prenatal Person, ch. 6), the most frequently used treatment for infertility in the developed world is In Vitro Fertilization followed by Embryo Transfer. The commercial aspects of this procedure can be best appreciated visiting the website of one of the centers that offer this treatment, for example: http://www.advancedfertility.com , the Advanced Fertility Center of Chicago. Note in particular the costs, the various "packages" available at different cost, and the extent to which the risks and side-effects of the treatment are described (or not mentioned). Try searching for GIFT on their site, (e.g.:https://www.advancedfertility.com/blastocyst.htm) and note how vigorously it is discouraged. Note also their solicitation for egg-donors of various ethnic backgrounds.
|
|
|
1. Harvesting egg and sperm 2. Fertilization 3. Incubation to blastocyst-stage (7-10 days) 4. Transfer of embryo to uterus |
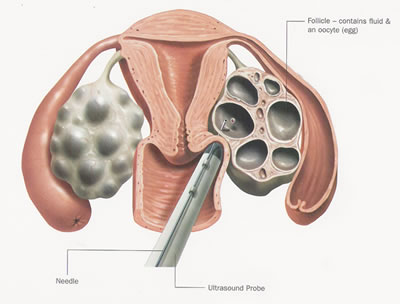
1.1 Retrieving Oocytes after
Ovarian Stimulation
|
|
|
| 1.1.1. Aspiration of a hyperstimulated ovary. | 1.1.2. Ultrasound probe locates stimulated follicle |
|
|
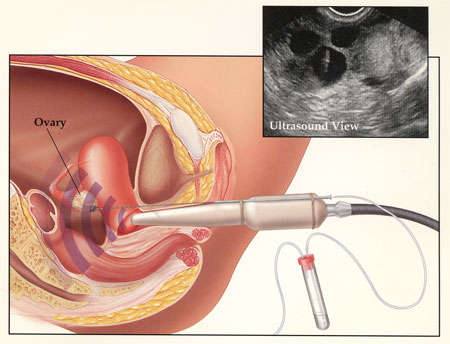
| 1.1.3. Aspiration of follicle. |
1.2.
Fertilization
|
|
| 1.2.1. Spermatazoa are mixed with the harvested oocytes. |
|
|
| 1.2.2. Artist's rendering of Intra-Cytoplasmic Sperm Injection |
1.3.
Incubation of
Embryos to
Blastocyst Stage
|
|
| 1.3.1. IVF Incubator |
|
|
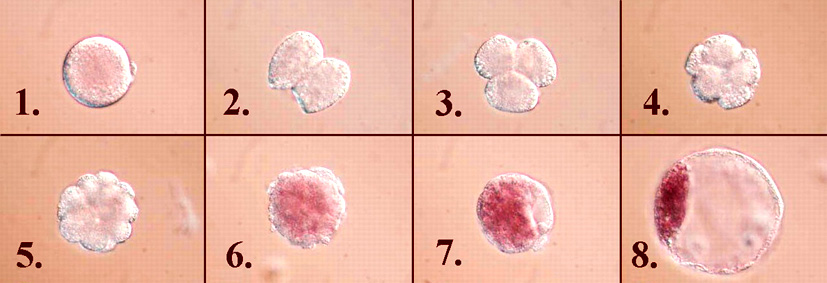
| 1.3.2. 1. Fertilized (bovine) oocyte; 5. Morula; 8. Blastocyst |
1.4.
Transfer of
Embryos
to the Uterus
|
|
| 1.4.1. Embryos transferred from syringe to uterus |
2.
THE
CATHOLIC
MAGISTERIUM
on In Vitro Fertilization
The moral significance and implications of in vitro fertilization were described in detail by the Congregation for the Doctrine of the Faith in the 1987 instruction, Donum Vitae. The intrinsically immoral nature of in vitro fertilization was reiterated, together with a specific condemnation of intracytoplasmic sperm injection, in the 2008 instruction, Dignitas Personae.
| II. The connection between in vitro fertilization and the voluntary destruction of human embryos occurs too often. This is significant: through these procedures, with apparently contrary purposes, life and death are subjected to the decision of man, who thus sets himself up as the giver of life and death by decree. This dynamic of violence and domination may remain unnoticed by those very individuals who, in wishing to utilize this procedure, become subject to it themselves. The facts recorded and the cold logic which links them must be taken into consideration for a moral judgment on IVF and ET (in vitro fertilization and embryo transfer): the abortion-mentality which has made this procedure possible thus leads, whether one wants it or not, to man’s domination over the life and death of his fellow human beings and can lead to a system of radical eugenics. | Nexus qui inter fecundationem in vitro et voluntariam peremptionem humanorum embryonum intercedit, nimio plus usu venit. Id est significationis plenum : hisce enim artibus, quamquam contraria appetuntur, mors et vita tandem in hominis voluntatem rediguntur, qui hoc modo se vitae necisque auctorem constituit, idque alieno iussu. Haec dynamica conexio violentiae ac dominii fortasse nec ab iis quidem percipitur, qui hisce artibus uti volentes, eisdem revera deserviunt. Quare tum facta supra memorata, tum illorum coniunctio, humanitatis expers, plane considerentur oportet, ut morale iudicium fiat de methodo FIVET (hoc est de fecundatione ovuli in vitro et de embryonis translatione) : nam mentis habitus proclivis ad abortum, qui tandem ad haec conduxit, inducit etiam, velimus nolimus, ad dominium hominis in vita ac morte proximorum, ex quo nasci potest « eugenismus » ad extremam formam adductus. |
|
[II.B.5] The Church remain opposed from the moral point of view to homologous ‘in vitro’ fertilization. Such fertilization is in itself illicit [intrisicus illicita] and in opposition to the dignity of procreation and of the conjugal union, even when everything is done to avoid the death of the human embryo. |
Ecclesiae iudicium perstat contrariurn fecundationi homologae in vitro: haec est intrinsecus illicita, ac dignitati procreattionis et coniunctionis coniugalis tunc etiam repugnat, cum illi omittitur ut embryonis mors praecaveatur. |
| Just as the Church condemns induced abortion, so she also forbids acts against the life of these human beings. It is a duty to condemn the particular gravity of the voluntary destruction of human embryos obtained ‘in vitro’ for the sole purpose of research, either by means of artificial insemination of by means of “twin fission”. | Quare Ecclesia, sicut abortum procuratum damnat, ita etiam prohibet, ne vita harum humanarum creaturarum attentetur. Conscientiae officium postulat, ut palam denuntietur peculiaris gravitas voluntariae interfectionis embryonum humanorum, qui in vitro obtenti sunt ad solum investigationis finem, ope sive fecundationis artificialis, sive <<fissionis gemellaris >> |
| By acting in this way the researcher usurps the place of God; and, even though he may be unaware of this, he sets himself up as the master of the destiny of others inasmuch as he arbitrarily chooses whom he will allow to live and whom he will send to death and kills defenceless human beings. | », quam vocant. Hac agendi ratione investigator se in locum Dei substituit atque, licet inconscius, se efficit dominum aliorum sortis, quippe qui arbitratu suo decernat quis vivat et quis morte afficiatur, idemque creaturas humanas interficiat, quae defensione carent. |
| II B 5. Homologous IVF and ET is brought about outside the bodies of the couple through actions of third parties whose competence and technical activity determine the success of the procedure. Such fertilization entrusts the life and identity of the embryo into the power of doctors and biologists and establishes the domination of technology over the origin and destiny of the human person. Such a relationship of domination is in itself contrary to the dignity and equality that must be common to parents and children. | Methodus FIVET homologa ad actum deducitur extra coniugum corpus, opera aliorum, a quorum scientia atque technica arte prosper exitus interventus dependet; eadem vitam identitatemque embryonum humanorum in potestatem redegit medicorum atque biologorum, sicque rei technicae dominatum quemdam in personae humanae originem et sortem instaurat. Huiusmodi dominatus suapte natura contradicit dignitati et aequalitati, quae parentibus et filiis communes esse debent. |
| Conception in vitro is the result of the technical action which presides over fertilization. Such fertilization is neither in fact achieved nor positively willed as the expression and fruit of a specific act of the conjugal union. In homologous IVF and ET, therefore, even if it is considered in the context of ‘de facto’ existing sexual relations, the generation of the human person is objectively deprived of its proper perfection: namely, that of being the result and fruit of a conjugal act in which the spouses can become “cooperators with God for giving life to a new person” | Conceptio in vitro est effectus actionis technicae, per quem evenit fecundatio ; ea autem neque re vera obtinetur, neque consulto appetitur tamquam manifestatio ac fructus actus qui est proprius coniunctionis coniugalis. In methodo FIVET homologa, igitur, etsi consideretur in contextu actuum coniugalium qui reapse exsistunt, nihilominus generatio personae humanae obiective destituitur perfectione sibi propria, qua scilicet illa est terminus et fructus actus coniugalis, per quem coniuges fieri possunt « Dei cooperatores tradendo vitae donum novo alicui homini )).*° |
2.2.
C.D.F. Dignitas Personae
(2008)
14. [...] all techniques of in vitro fertilization proceed as if the human embryo were simply a mass of cells to be used, selected and discarded. [...]15. the number of embryos sacrificed is extremely high. [...] in many cases the abandonment, destruction and loss of embryos are foreseen and willed [...] the practice of multiple embryo transfer implies a purely utilitarian treatment of embryos.
16. The blithe acceptance of the enormous number of abortions involved in the process of in vitro fertilization vividly illustrates how the replacement of the conjugal act by a technical procedure – in addition to being in contradiction with the respect that is due to procreation as something that cannot be reduced to mere reproduction – leads to a weakening of the respect owed to every human being.
17. Intracytoplasmic sperm injection (ICSI) is morally illicit, [in that it] causes a complete separation between procreation and the conjugal act”
THESE condemnations represent the application of principles earlier enumerated concerning the control and domination of nature in general and of human reproduction in particular:
2.3.
Pope Saint Paul VI,
Humanæ Vitæ:
(1968)
|
2.[4] Finally, and above all, it must be noted that
because Man has made such remarkable progress in
controlling
[moderandis]
the forces of nature and in rationally organizing them,
he also strives to extend this
control
[moderationem]
to the whole of his life: that is, to his body, to the powers of his
mind
[ad sui animi vires],
to his social
life, and even to the laws that regulate the propagation of life. |
Denique illud praesertim animadvertendum est, hominem tam mirifice profecisse in naturae viribus cum moderandis tum ad rationem scite componendis, ut hanc moderationem ad totam suam vitam proferre conetur : hoe est, ad suum corpus, ad sui animi vires, ad vitam socialem, ad ipsasque leges propagationem vitae regentes. |
|
17.
Therefore, if we do not want the mission [officium]
of procreating human life to be conceded to the arbitrary decisions of
Men, we need to recognize that there are some limits to the power of Man
over his own body and over the natural operations [munera]
of the body, that ought not to be transgressed. No one, neither a private
individual nor a public authority, ought to violate these limits. For
these limits are derived from the reverence owed to the whole human body
and its natural operations [naturalibus muneribus],
according to the principles acknowledged above, and according to a proper
understanding of the so-called principle of totality, as explained by Our
Predecessor, Pius XII.47 |
Quare, nisi velimus ut procreandae vitae officium hominum arbitratui concedatur, necessario aliquos fines, quos ultra progredi non liceat, agnoscamus oportet illi potestati, quam homo in proprium corpus in eiusque naturalia munera habere potest; fines, dicimus, quas nemini, sive privato sive publica auctoritate praedito, violare licet. Qui limites non aliam ob causam statuuntur, quam ob reverentiam, quae toti humano corpori eiusque naturalibus muneribus debetur, secundum principia, quae supra memoravimus, et rectam intellegentiam principh totalitatis, ut aiunt, quod Decessor Noster v. m. Pius XII illustravit. |
|
21. Moral family
planning requires that spouses recognize and value the true goods of life
and the family, and also that they acquire the habit of
complete
mastery
[moderari]of themselves and their desires
[motibus].
In order to control the drives of
nature, the spouses need to become self-denying
[asceseos] through using their reason and free will.
Only then will the manifestations of love appropriate for married couples
be what they ought to be. Self-mastery is especially necessary for those
who practice periodic abstention. |
21. Recta autem et honesta nasciturae prolis ordinatio id primum a coniugibus postulat, ut vera vitae familiaeque bona penitus agnoscant et existiment, itemque sibi ac suis motibus perfecte moderari consuescant. Nihil profecto est dubii, quin naturae impetibus, rationis liberaeque voluntatis ope, imperare asceseos sit opus, ut nempe amoris significationes, coniugalis vitae propriae, cum recto ordine congruant; quod praesertim ad usum continentiae, certis temporis intervallis servandae, requiritur. |
2.4.
Pope Saint John Paul II,
The Theology of the Body
(1984):
6. [119] General Audience of 22 August 1984, [Ws. 123, pp. 630-633; ToB 396-399]
1. [...] This extension of the sphere of the means of “domination of the forces of nature” menaces the human person for whom the method of “self-mastery” is and remains specific. The mastery of self corresponds to the fundamental constitution of the person; it is indeed a “natural” method. On the contrary, the resort to artificial means destroys the constitutive dimension of the person. It deprives man of the subjectivity proper to him and makes him an object of manipulation.
2.5.
Pope Saint John Paul II,
Evangelium Vitae
(1995):
|
“Be fruitful and multiply, and fill the
earth and subdue it” |
“Crescite et multiplicamini et replete terram et subicite eam” (Gen. 1, 28): hominis de vita officia |
|
42. [...]As one called to till and look after the garden of the world (cf. Gen 2:15), [...] |
42.Ad mundi hortum colendum tutandumque vocatus (Cfr. Gen. 2, 15) [...] |
|
“the dominion granted to man by the Creator is not an absolute power, nor can one speak of a freedom to ‘use and misuse’, or to dispose of things as one pleases. The limitation imposed from the beginning by the Creator himself and expressed symbolically by the prohibition not to ‘eat of the fruit of the tree’ (cf. Gen 2:16-17) shows clearly enough that, when it comes to the natural world, we are subject not only to biological laws but also to moral ones, which cannot be violated with impunity”.[2] |
“dominium a Creatore homini datum... non est absolutum, nec potest utendi et abutendi arbitrium vocari, vel ex commodo res disponendi. Modus, quem inde a principio ipse Creator homini imposuit quique symbolica ratione exprimitur per interdictionem comedendi de ligno (Cfr. Gen. 2, 16-17), satis clare ostendit in universitate naturae visibilis... nos legibus esse subiectos, non solum biologicis, verum etiam et moralibus, quae impune violari nequeunt” (IOANNIS PAULU PP. II Sollicitudo Rei Socialis, 34). |
|
|
|
|
|
|
3. COMPLICATIONS
and SIDE
EFFECTS
of In Vitro Fertilization
The subject of complications and side-effects of In Vitro Fertilization and Embryo Transfer is complex and controversial. Identical scientific studies are often cited by individuals who hold opposing points of view, one side claiming that IVF is safe for mother and offspring, with the other maintaining that the same studies deminstrate significant morbidity for both mothers who use IVF and for their resultant children. The following side-effects are well-documented and indisputable.
3.1 Ovarian Hyperstimulation Syndrome
The drugs (gonadatropins) used to induce multiple simultaneous ovulations can cause “ovarian hyperstimulation syndrome,” a potentially dangerous condition that can cause edema (fluid retention) and death.
[...] significant ovarian hyperstimulation syndrome (OHSS) occurs in approximately 0.5% of women receiving gonadotropins. OHSS can be life-threatening, causing massive fluid shifts, ascites, pleural effusion, electrolyte disturbances, and thromboembolism.
Lentz, G., Comprehensive Gynecology, 6th ed. ( 2012, Mosby, Elsevier). p. 882
Supporters of IVF claim that lower doses of the drugs used to stimulate the ovaries can avoid this complication; however the lower dose-regimen results in the production of fewer eggs, and may necessitate more cycles of IVF.
It is accepted that excessive ovarian stimulation leads to the risk of hyperstimulation and a poor outcome, including the possibility of oocyte aneuploidy and a disordered endometrium. Nevertheless, obtaining an adequate number of mature oocytes leads to having more embryos available for transfer and possible cryopreservation.
Lenz, Comprehensive Gynecology, 6th ed. (2012), p. 892
In July of 2012 an article was published in the New York Times on Ovarian Hyperstimulation in fertility treatment.
3.2. Birth Defects
Studies that have demonstrated an increased incidence of birth defects associated with IVF have been interpreted by some as an indictment of the practice of Intracytoplasmic Sperm Injection (ICI), rather than reflecting some more fundamental flaw in the overall practice of IVF. It is possible that defective sperm which would otherwise been incapable of effecting fertilization are sometimes introduced into the harvested oocytes by ICI. Other factors that increase the incidence of birth defects include advanced maternal age and multiple gestation (twins, triplets, quadruplets, etc.), as described in the next section.
3.3 Multiple Gestations
A frequent complication of IVF is multiple gestation, the situation in which a woman finds herself pregnant with more than one child. In order to increase the likelihood of pregnancy following IVF, multiple embryos are invariably created: some are transferred to the mother, while others are frozen against possible future need. If all the embryos successfully implant and develop, there is risk, not only to the mother, but to the infants themselves:
Women pregnant with multiples not only have higher risks for developing certain conditions but also are more likely to have more severe manifestations of those conditions
Gabbe, S., Obstetrics: Normal and Problem Pregnancies, 6th ed.. (2012 Saunders, Elsevier), p. 667.
Babies who are products of multiple gestations have higher rates of low birthweight, earlier gestational age at delivery, and higher rates of neonatal and infant death and cerebral palsy.
Gabbe, S., Obstetrics, 6th ed.. (2012), p. 678.
4.
REPRESENTATIVE
RECENT
ARTICLES
on BIRTH
DEFECTS
and
In Vitro Fertilization
4.0. A
multi-centre cohort study of the physical health of 5-year-old children
conceived after intracytoplasmic sperm injection, in vitro fertilization and
natural conception.
M. Bonduelle, U.-B. Wennerholm, et.
al. Human Reproduction v.20, 2004, Issue 2, 413-419.
BACKGROUND: Over a million children have been born from assisted conception worldwide. Newer techniques being introduced appear less and less ‘natural’, such as intracytoplasmic sperm injection (ICSI), but there is little information on these children beyond the neonatal period.
METHODS: 540 ICSI conceived 5-year-old children from five European countries were comprehensively assessed, along with 538 matched naturally conceived children and 437 children conceived with standard IVF.
RESULTS: Of the 540 ICSI children examined, 63 (4.2%) had experienced a major congenital malformation. Compared with naturally conceived children, the odds of a major malformation were 2.77 (95% CI 1.41–5.46) for ICSI children and 1.80 (95% CI 0.85–3.81) for IVF children; these estimates were little affected by adjustment for socio-demographic factors. The higher rate observed in the ICSI group was due partially to an excess of malformations in the (boys') urogenital system. In addition, ICSI and IVF children were more likely than naturally conceived children to have had a significant childhood illness, to have had a surgical operation, to require medical therapy and to be admitted to hospital. A detailed physical examination revealed no further substantial differences between the groups, however.
CONCLUSIONS: Singleton ICSI and IVF 5-year-olds are more likely to need health care resources than naturally conceived children. Assessment of singleton ICSI and IVF children at 5 years of age was generally reassuring, however, we found that ICSI children presented with more major congenital malformations and both ICSI and IVF children were more likely to need health care resources than naturally conceived children. Ongoing monitoring of these children is therefore required.
4.1.
In vitro fertilization and risk of
childhood leukemia in Greece and Sweden.
Petridou, E.T., Pediatr Blood Cancer,
01-JUN-2012;
58(6): 930-6.
BACKGROUND: Cancer risk in children born after in vitro fertilization (IVF) remains largely unknown. We aimed to investigate risk of leukemia and lymphoma following IVF using two nationwide datasets.
METHODS: The hospital-based case-control study in Greece derived from the National Registry for Childhood Hematological Malignancies (1996-2008, 814 leukemia and 277 lymphoma incident cases with their 1:1 matched controls). The Swedish case-control study was nested in the Swedish Medical Birth Register (MBR) (1995-2007, 520 leukemia and 71 lymphoma cases with their 5,200 and 710 matched controls) with ascertainment of incident cancer cases in the National Cancer Register. Study-specific and combined odds ratios (OR) were estimated using conditional logistic regression, with adjustment for possible risk factors.
RESULTS: Nationwide studies pointed to similar size excess risk of leukemia following IVF, but to a null association between IVF and lymphoma. The proportion of leukemia cases conceived through IVF was 3% in Greece and 2.7% in Sweden; prevalence of IVF in matched controls was 1.8% and 1.6%, respectively. In combined multivariable analyses, the increased risk of leukemia was confined to age below 3.8 years (OR 2.21; 95% confidence interval, CI: 1.27-3.85) and to acute lymphoblastic leukemia (ALL) (OR 1.77; 95% CI: 1.06-2.95) with no sufficient evidence of excess risk for other leukemias (OR 1.34; 95% CI: 0.38-4.69). Following IVF, OR for ALL was 2.58 (95% CI: 1.37-4.84) before age 3.8 and 4.29 (95% CI: 1.49-12.37) before age 2 years.
CONCLUSIONS: IVF seems to be associated with increased risk of early onset acute lymphoblastic leukemia in the offspring.
4.2. Cancer risk in children and
young adults conceived by in vitro fertilization.
Källén, B., Pediatrics
- 01-AUG-2010;
126(2): 270-6
4.3.
Birth defects in children conceived by in vitro fertilization and
intracytoplasmic sperm injection: a meta-analysis
Juan Wen, Jie Jiang, et.al.
Fertility and Sterility, June 2012 Volume 97, Issue 6, 1331–1337
http://www.fertstert.org/article/S0015-0282(12)00287-7/abstract?cc=y=
4.4.
Risk of birth defects in children conceived with assisted reproductive
technology: A meta-analysis
Lu, Yue; Liu, Lele, et. al.
Medicine 101(52):p e32405, December 30, 2022.
BACKGROUND: Although assisted reproductive technology (ART) is extensively used in couples with fertility problems, the risk of birth defects among infants conceived with ART is still a concern. Therefore, to more accurately assess the risk of birth defects after ART treatment, we performed a meta-analysis of all available cohort studies relating to birth defects among infants conceived with ART.
METHODS: We used an established strategy to search the databases of PUBMED, EMBASE, COCHRANE, WEB OF SCIENCE, CNKI, CBM and VIP for studies published between 2008 and 2020. Subgroup analyses and sensitivity analyses were used to examine sources of heterogeneity. Pooled adjusted odds ratios (ORs) were calculated using a fixed effects model. RevMan5.3 was used to draw a forest plot, and Stata14.0 was used to test for publication bias.
RESULTS: We included 14 cohort studies from different countries. The infants conceived with ART had a 1.22-fold higher likelihood of birth defects than children born after natural pregnancy(OR = 1.22, 95% CI [1.17, 1.28], P < .05). The prevalence of birth defects after ART treatment was higher in singleton births than in multiple births. In a meta-analysis of data from 6 studies, we found associations between ART and birth defects related to specifics organs: cardiovascular defects, OR = 1.51, 95% CI [1.34–1.69], P < .05; musculoskeletal defects, OR = 1.09, 95% CI [1.03–1.15], P < .05; urogenital defects, OR = 1.24, 95% CI [1.11–1.38], P < .05; central nervous system defects, OR = 1.33, 95% CI [1.14–1.55], P < .05; and orofacial defects, OR = 1.45, 95% CI [1.15–1.83], P < .05.
CONCLUSIONS: ART treatment does present an increased risk of birth defects. The prevalence of birth defects after ART treatment is lower in multiple births than in singleton births. Further research is required to examine the risks for birth defects after ART treatment.
I SOLD
MY
EGGS
for an IVY
LEAGUE
EDUCATION
–
BUT
WAS
IT
WORTH
IT?
THE
GUARDIAN: Sun 7 Nov 2021
https://www.theguardian.com/lifeandstyle/2021/nov/07/i-sold-my-eggs-for-an-ivy-league-education-but-was-it-worth-it
An increasing number of women are
selling their eggs
for as much as $20,000 a cycle to cover essential costs
by Ellie Houghtaling
MY eyes flutter open. I’m surrounded by four nurses holding me upside down. They shake me back and forth, urging the blood back to my head. As I regain consciousness I wonder: is this worth it? That “it” is the $10,000 question.
Seven months ago, I received my acceptance to Columbia University’s School of Journalism. I was absolutely stunned to be admitted, but even more shocked by the $116,000 price tag – and that was just for tuition. The school, whose education is widely considered the golden standard in journalism, would provide me with unparalleled access, in an industry I currently felt immobile in.
Fortunately, the vast majority of the cost would be covered by scholarships. For the remaining rent and living costs, I looked for something else to plug the gap. I landed on a burgeoning industry offering struggling people vast amounts of cash, relatively fast: egg donation.
It’s 90-something degrees on a June morning in New York City. My wrinkled, green satin skirt sticks to my legs as I rush into the egg donation clinic’s main office for another screening, a urine test.
Over the last four months I’ve been lying to my somewhat conservative family about where I’ve been escaping to on these early mornings: surreptitiously showing up for examinations and psychological assessments in order to donate my eggs.
Outside of my family, I’ll more often say I’m “selling my eggs”. Donation is a term that is supposed to reflect that it’s a woman’s time, not the value of her eggs, that’s being paid for. But here was an industry offering me more per hour than I’d ever earned at a regular job. To say I’m selling feels more honest.
In the clinic’s main office, Amy Winehouse’s deep voice plays softly on a nearby speaker. Looking around the waiting room, with its lavender and gray accents splashing the walls, I quickly realize I’m the only woman sitting alone. I share fleeting glances with giggling couples and wonder if any of them are sizing me up as a possible donor.
I wasn’t the patient. I was the product
Sometime after my arrival, a nurse calls my name. Amy Winehouse’s harmonies fade away. She takes me to a chair in a hallway: a dozen or so vials clinking around on an attached tray. The space feels cold and sterile. The silence is oppressive. I try to remember if I ate breakfast – I didn’t.
A nurse scoots over and pulls my arm over the cuff of the chair.
“Beautiful veins,” she says.
After she has filled eight or so vials with my blood, I slump over and pass out. When I awake, the nurses have swept me into the air. Semi-conscious, and embarrassed I stumble over an apology.
I’m escorted to a gynecological chair in a nearby examination room and given a pineapple flavored lollipop. I lean my head back against the cold chair. Another nurse walks in, showing off more vials in her hand. I roll up my sleeve and hold out my other arm. Time for round two.
Ifirst called the egg donation clinic back in March 2021 – moments before I attended Columbia Journalism School’s introduction day. The first time I heard of donation was through a friend during my undergraduate studies. I knew I couldn’t risk the distraction and stress of a job while studying at Columbia full-time. Plus, the school’s administration reminded us outright that we were to avoid employment during our studies.
The Google search that led me to my new career choice was simple: “Egg donation agencies in New York City.” I’m not the only one to type it. Every year, donors are being paid in the thousands to provide eggs to prospective parents. The CDC found that in under a decade, IVF cycles using donor eggs nearly tripled, from roughly 5,000 in 2007 to more than 13,000 in 2016.
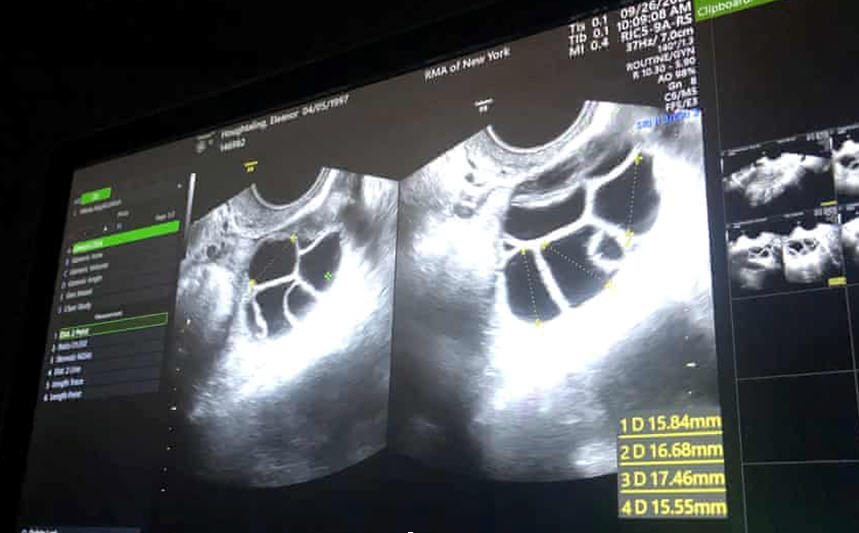
The woman on the phone was cheery but meticulous when she described the process. In contrast, my first visit to the clinic’s SoHo office was impersonal. During my ultrasound, awe-struck as I gazed into the contents of my ovaries and uterus, my doctor spoke about me to the nurse, but not to me.
|
|
Scans of my ovaries show expanding antral follicles, doubled and tripled in size, after nearly two weeks of hormone therapy. Photograph: Ellie Houghtaling
In a traditional doctor-patient relationship, the doctor’s bedside manner is fundamental. In the US – where healthcare is privatized and people weigh up doctors as if their health were a business transaction – medical offices treat you well because they want you to come back. My first day in SoHo made me realize that this time, I wasn’t the patient. I was the product.
The bloodwork from that first appointment was sent off to a genetic testing facility, Sema4, which tested 283 of my genes against hundreds of disorders. Those ranged from cystic fibrosis and Fragile X syndrome – which has been connected to autism – to maple syrup urine disease, a disorder where the body cannot process certain amino acids.
I tested positive as a carrier for three genetic conditions: dystrophic epidermolysis bullosa – a condition that creates skin so fragile that it blisters and breaks easily, leaving severe scarring; metachromatic leukodystrophy – a rare genetic disorder; and non-syndromic hearing loss. I felt a mixture of shock and morbid curiosity hearing the results, though the clinic reassured me it was normal to test positive for a small handful of genetic disorders.
Epidermolysis bullosa has no cure, and people born with the condition are at increased risk for an extremely aggressive form of skin cancer. The Sema4 representative playfully told me not to fall in love with Finnish people, who are more likely to have the same skin condition.
They would compliment my body, personality and ivy league education. I had concerns this was sanitized eugenics.
The call offered a window into a different world: where everybody is a carrier of disease, myself included. I was forced to confront a reality where I might pass on complex disorders to my children, ones I never thought I had.
The clinic was not just assessing my predisposition for genetic disorders, it was also weighing up other attributes: my blonde hair, my blue eyes and my fair skin. Over screening calls, team members would subtly compliment and affirm descriptions of my body, personality and ivy league education. Altogether, I had concerns this was sanitized eugenics. But through what other language did I expect them to build a relationship with me? They were paying me $10,000 for my eggs. The very nature of our business revolved around my body.
In May, early on in the process, the clinic set me up to speak with their psychologist. Lounging in the hammock on my balcony, I was exposed to the philosophy of the clinic. My eggs weren’t “mine” and “my eggs” were certainly not synonymous with “my child”. Rather, they saw my eggs as a part of a larger gene pool, one that spanned generations and geographic locations.
I was concerned the psychologist was assessing my mental health, looking to disqualify me from the process, but as our conversation flowed I realized she was actually trying to ascertain whether I was intelligent enough to make the decision to give away my eggs. She gave me an IQ test. It was New York state regulation.
The idea that my eggs weren’t “mine” but rather some genetic tie to the past struck me as odd and uncomfortable at first, but over time I grew to prefer that framing to my own. I wasn’t giving up “my” child - I was giving up another period. This would help struggling parents conceive children of their own. There was something wholesome about that.
The idea that a small child, that looked like me would roam the world while I experienced my early twenties never fazed me. The thought actually warmed my heart.
I grew to realize I wanted children of my own one day, and part of me yearned for the experience I was offering to someone else. I imagined the mom who would take my eggs.
Was she funny? What kind of school lunches would she pack? Was she compassionate and patient? Would she hold the child’s hand often? Did her moral values reflect my own? I would never know. My donation was anonymous end-to-end.
By summertime, the clinic had taken me off of my birth control and put me on their own. One morning when I went to their office to collect an envelope of the beige pills, the nurse handing them to me apologized, saying she didn’t understand why it was taking so long to match me with a family.
“You’re a hot commodity,” she said.
We paused for a moment, staring at one another. My hair had fallen in front of my eyes. I pushed the dirty blonde strands back behind my ear before erupting in uncomfortable laughter. We both knew what she meant.
A few days away from my egg retrieval date I was sitting on the edge of my bed feeling truly unsettled. It was late, and in the quiet I felt the calm ripped away from me as I laid out one of the last packs of medication, a 250 microgram syringe of Ganirelix, on my table stand.
It took some mental gymnastics to learn to inject myself with hormones twice daily. Each medication had a different ritual. In the morning, a yellow and blue plastic pen would deliver 225 ml of Follistim, clicking as I pushed the pen down to dispense the refrigerated serum. In the evenings, I would mix a vial of Menopur. Combined, these two drugs worked to stimulate the follicles in my ovaries, aiming to release anywhere between 10-20 eggs – normally, just one egg is released during ovulation.
Days before retrieval, Ganirelix would prevent me from ovulating, giving the eggs a chance to mature before they descended into my uterus to be removed.
This final stage numbed me. The rigamarole of daily injections and 7 am ultrasounds had worn me down, and I was tired. On the horizon, I still had one more hurdle: retrieval. I ran my hand over my stomach, feeling the tender needle sites and the bloat underneath, not wanting to undergo the surgery but also knowing it was too late to turn back. I grabbed my first syringe of Ganirelix and took a deep breath.
Isurveyed a dozen women of varying ages and backgrounds on their personal experiences donating. Unlike infertility forums for people going through IVF or surrogacy, there was no clear online location where donors could support each other through the process of egg donation. Instead, I found them scattered across private Facebook groups, WhatsApp chats and Reddit.
Most donated during their early twenties and all participated for the financial compensation, at least originally. There was a pay scale, largely determined by geographic location and time of donation, ranging from $3,000 to $20,000. Women used the money to pay for bills, student loans or vacations.
Some donors matched with intended parents or agencies through advertisements placed on Facebook or Instagram. Others found their matches on Craigslist, responding to blanket ads not dissimilarly phrased to those looking to sell a bicycle, apartment or car.
“JEWISH WOMEN --- Earn $10,000 with the Gift of Egg Donation”
“Chinese, Vietnam, Korean, Asian Egg Donors Earn $10,000”
“Seeking a Highly Intelligent Egg Donor! Compensation up to $40K”
Since these listings are sometimes posted directly by the intended parents, they may have shorter or less thorough initial application processes, and they can offer significantly higher monetary sums than agencies or clinics traditionally would. But applying to unverified listings poses obvious risks. In 2011, an Idaho woman was charged with fraud for stealing eggs from donors through Craigslist, never paying the agreed upon sums after receiving the eggs.
Attempting, in part, to make the process safer, organizations began pairing donors and intended parents through their own vetted databases. Prospective parents, can now scroll through the profiles of thousands of potential donors, not unlike on a dating website. Circle Surrogacy offers non-anonymous pairings, where the donor has an opportunity to meet and interact with the families.
Jordan Whaley Finnerty’s profile features an image of her then five-year-old daughter – all smiles beside her mom. Whaley set it up when she was 27.
That was in 2018, after a wine night with a friend who had just undergone a donation herself – Finnerty was intrigued, especially by the $9,000 lump sum. She wasn’t desperate for the money, but she knew it would help her stop living paycheck to paycheck. She applied that night and forgot about it.
“Four months later I was donating,” Finnerty said.
Since then, Finnerty has donated four times.
“It wasn’t until I was matched with a family, met them, [and] spoke with them that I realized the impact,” said Finnerty. “You don’t realize the lengths couples have to go through to have children.” She’s had contact with all of the families she’s donated to. Being exposed to the parents’ gratitude changed her mind. Now, the goodwill of element, not the money, is her favorite part: She plans to donate six times – the maximum advisable.
Still, she acknowledges certain issues in the industry.
“Speaking with intended parents, they express how weird it is to be going over girls’ profiles and looking into their health history, basing their preferences off of hair color or eye color,” Finnerty told me over Facebook one evening.
But she also knows that people make these choices with their partners all the time.
To prevent people from donating repeatedly (with the risks being unknown), or incentivizing people to withhold information to make themselves more attractive to donors, ethical guidelines suggest offering less money.
In a recent opinion published by American Society for Reproductive Medicine – which dissuades agencies from compensating donors more than $10,000 – the society found that 88% of donors compensated up to $5,000 for their eggs answered in a self-report questionnaire that “being able to help someone” was their biggest motivation.
“I think [people assume] there’s a sense of coercion out there, but there’s really none of that,” said Deborah Mecerod who runs MyEggBank, the largest egg donation bank network in the US. Their policy is to offer one flat-fee as payment, capped at $10,000. Mecerod feels the experience is very rewarding for prospective donors, through the education and free genetic testing, even if they choose not to follow through with the donation. “There’s always the option to leave the process,” she said.
While many women admit to being pulled in by the amount they can earn from their eggs, most I spoke to still saw it as a choice.
“The first and second time I was unemployed or barely employed, so in a way [I needed the money] but I wasn’t desperate for it,” explains Dolan Wells Gallagher, who has now donated her eggs three times. The first and second time she used the money to cover rent while she was between jobs, the third time, to pay tuition fees.
Data and long-term research on egg donation is scarce. In 2016, new research suggested that fertility drugs may be linked to the development of uterine cancers. A 2017 report by The Donor Sibling Registry found suspicious occurrences of breast cancer in otherwise healthy young donors who showed no genetic predisposition to the disease, citing hormone therapy during donation as a possible cause. “The lack of information may be misleadingly interpreted as lack of risk,” the report warned.
Four years later, there’s still no semblance of a long-term database to monitor the health of donors. Furthermore, while health data is monitored for those who donate organs, the same information is not required for egg donation: it is up to donation agencies to request past medical information on donors, and even then they are at the mercy of donors voluntarily doing so – and telling the truth when they do. Most are not asked for, and do not report, medical changes after starting the process.
In the meantime, thousands of young donors every year undergo egg removal and hormone treatment, without anyone fully understanding the consequences.
“Having a donor registry would be such a great tool for so many different reasons, because you could collect data from the donor, how she’s doing and follow up in years to come,” explains Mecerod, who believes legislation and federal government intervention would help solve this problem.
But most women I interviewed didn’t seem too bogged down by the ramifications of long-term health complications. Most of them needed the money. When the cycle ends, the donors leave with the future impacts a mystery.
Up until the very end of my first donation, I felt positive about my experience. Despite fainting; feeling objectified and shuffled around; despite the laborious injections, I still liked it. I felt comfort and satisfaction knowing I helped people achieve their dreams.
But in the final days ticking down to my surgery, I felt a slew of emotions that confused what I thought would be a rewarding end.
I felt at the mercy of the clinic. Appointments were made at locations I’d asked not to be sent to, because they were out of my way. Some days I didn’t receive updates about how much medication I should take, leaving me to take a stab in the dark at the dosage. I didn’t find out when my surgery would be until two days before the event.
I wonder if the woman receiving my eggs is more informed than I am
On the day before my surgery, I asked a nurse point-blank why they scheduled surgeries with such little advance. She didn’t know. I felt disrespected and angry. The company was inconsiderate of my time, and I was suddenly left scrambling around to make sure someone could still pick me up from my surgery the following day.
I was expected to have absolute flexibility. Appointments popped up and I was expected to be available. As the week wore on, my enlarged ovaries sat heavy in my abdomen as a thick and uncomfortable reminder.
After my final appointment on Tuesday, I wrote in my journal: “At this stage I genuinely do feel left in the dark and I don’t really want to deal with these people anymore. I wonder if the woman receiving my eggs is more informed than I am.”
Still, I looked forward to receiving the $10,000 check. Life in New York, one of the world’s most expensive cities, took unexpected tolls on my wallet on a daily basis. The arrival of this check would quell my anxiety for a handful of months, allowing me to return to my studies stress-free – studies which would offer me stability and confidence towards my dream job. Every piece was a steppingstone towards a future I desperately wanted.
My surgery lasted a total of seven minutes and laid me up in bed for a day and a half at home, as my stomach cramped and contorted. The clinic offered me no pain relievers, so I lived on a cocktail of Tylenol and Advil. Fortunately, my pain wasn’t too bad. Reflecting on the procedure as a whole, I jotted down a couple lines in my journal:
“I would consider doing this again. I do worry about how it would impact my body, but the impact on my life would be so significant. I don’t know if I could deny that.”
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002