|
|
|
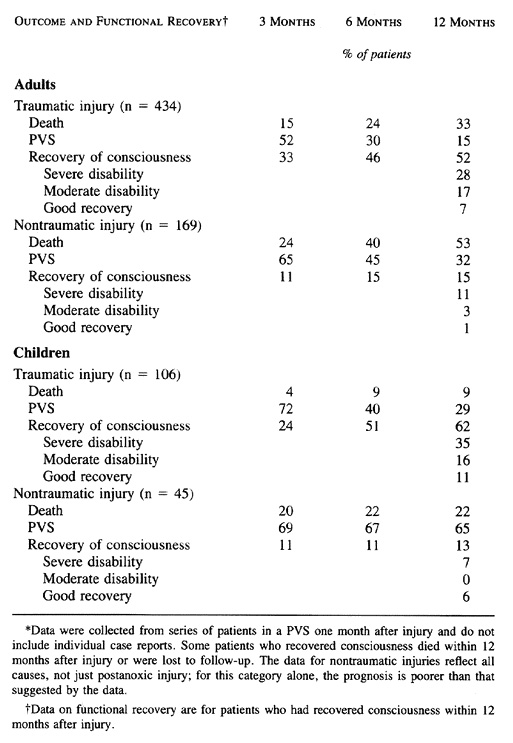
Table 3. Incidence of Recovery of
Consciousness and Function in Adults and Children in a Persistent Vegetative
State (PVS) after Traumatic or Nontraumatic Brain Injury |
PERSISTENT VEGETATIVE STATE
|
|
|
Table 3. Incidence of Recovery of
Consciousness and Function in Adults and Children in a Persistent Vegetative
State (PVS) after Traumatic or Nontraumatic Brain Injury |
|
|
|
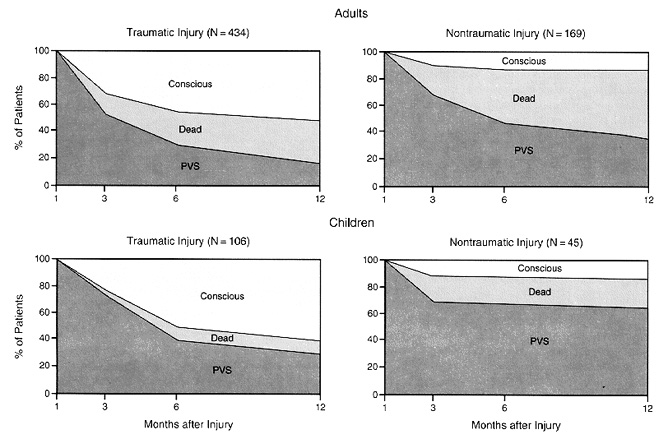
Figure 1.
Outcome for Patients in a Persistent Vegetative State (PVS) after a
Traumatic or Nontraumatic Injury.
Fifty-two percent of adults and 62 percent of children who are in a PVS one
month after a traumatic injury recover consciousness within one year. The
majority recover within the first six months; recovery after six months is
unusual. In contrast, for patients in a PVS one month after a nontraumatic
injury, recovery of consciousness is much less frequent (15 percent of
adults and 13 percent of children) and is extremely unlikely after three
months. Approximately 5 percent of patients in a PVS 1 month after injury
were lost to follow-up at 12 months |
The term "persistent vegetative state" was coined by Jennett and Plum in 1972 to describe the condition of patients with severe brain damage in whom coma has progressed to a state of wakefulness without detectable awareness1. Such patients have sleep-wake cycles but no ascertainable cerebral cortical function. Jennett and Plum thought that patients in a persistent vegetative state could be distinguished clinically from those with other conditions associated with prolonged unconsciousness.
In 1983 the President's Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research accepted the definition of persistent vegetative state proposed by Jennett and Plum and defined unconsciousness as the inability "to experience the environment." In the commission's judgment, a persistent vegetative state is only one form of permanent unconsciousness2. The others include coma after a traumatic or nontraumatic injury, with death occurring before the recovery of sufficient brain-stem function to allow a stable vegetative state; the end stages of degenerative neurologic conditions, such as Alzheimer's or Creutzfeldt-Jakob disease; coma from untreatable mass lesions such as neoplasms or vascular masses; and anencephaly in infants.
Because of the diagnostic, prognostic, and therapeutic uncertainties concerning the persistent vegetative state, several professional medical organizations began a comprehensive examination of their standards of medical care for patients with this condition3,4,5,6,7. In 1989, the American Academy of Neurology published a position paper that defined persistent vegetative state, classified artificial nutrition and hydration as forms of medical treatment, and stated that patients or their surrogates could decide to terminate treatment and that there were no medical or ethical distinctions between withholding and withdrawing treatment8. A 1990 survey by the American Neurological Association found that 88 percent of responding members agreed with this document9. In a 1991 survey by the Child Neurology Society, 92 percent of respondents agreed with the position paper as it related to adults, but only 72 percent thought that it was applicable to infants and children10. In addition, 75 percent of the respondents to this survey indicated that they would not withdraw nutrition and hydration from children in a persistent vegetative state.
In 1990, the Council on Scientific Affairs and the Council on Ethical and Judicial Affairs of the American Medical Association issued a report that provided clinical criteria for the diagnosis of a persistent vegetative state and discussed ethical and legal implications of decisions to withhold or withdraw life-prolonging medical treatment -- matters that were receiving widespread attention at the time11,12,13,14,15. In 1991, the United Kingdom's Institute of Medical Ethics Working Party on the Ethics of Prolonging Life and Assisting Death published a position statement indicating that a diagnosis of persistent vegetative state could usually be made with confidence three months after the acute insult but that in young children, the extent of damage and period of recovery were less predictable16. More recently, the British Medical Association's Medical Ethics Committee and the American Neurological Association have published position papers that define criteria for the clinical diagnosis of a persistent vegetative state and address several of the ethical issues concerning the care of patients in such a state17,18.
Because of the acceptance of recent consensus statements concerning guidelines for determining brain death in children19 and the medical aspects of anencephaly in infants,20 the Multi-Society Task Force on PVS was established in 1991 and charged with the creation of this document. Two representatives were appointed from each of the five societies, and an advisory panel of consultants was selected from the related fields of medicine, ethics, and law. The document was approved by the executive committee of each society.
Data reviewed by members of the task force were obtained from several sources, including a comprehensive literature review of all Medline references to the terms "vegetative state" and "persistent vegetative state," a "request for information" published in medical journals supported by the five sponsoring societies, a review of stories in the popular media concerning unexpected recovery from prolonged coma, and data from the National Institute of Neurological Disorders and Stroke Traumatic Coma Data Bank.
This statement by the task force summarizes the medical facts about the persistent vegetative state; it does not address associated ethical, legal, or other issues. The statement is divided into two parts. The first defines persistent vegetative state and related terms and conditions and discusses the epidemiology, causes, and pathological features, as well as ancillary diagnostic studies. The second part addresses the prognosis for recovery and long-term survival of patients in a persistent vegetative state and discusses issues related to pain and suffering and treatment.
Definition and Clinical Aspects
The vegetative state is a clinical condition of complete unawareness of the self and the environment, accompanied by sleep-wake cycles with either complete or partial preservation of hypothalamic and brain-stem autonomic functions. The condition may be transient, marking a stage in the recovery from severe acute or chronic brain damage, or permanent, as a consequence of the failure to recover from such injuries. The vegetative state can also occur as a result of the relentless progression of degenerative or metabolic neurologic diseases or from developmental malformations of the nervous system.
The vegetative state can be diagnosed according to the following criteria: (1) no evidence of awareness of self or environment and an inability to interact with others; (2) no evidence of sustained, reproducible, purposeful, or voluntary behavioral responses to visual, auditory, tactile, or noxious stimuli; (3) no evidence of language comprehension or expression; (4) intermittent wakefulness manifested by the presence of sleep-wake cycles; (5) sufficiently preserved hypothalamic and brain-stem autonomic functions to permit survival with medical and nursing care; (6) bowel and bladder incontinence; and (7) variably preserved cranial-nerve reflexes (pupillary, oculocephalic, corneal, vestibulo-ocular, and gag) and spinal reflexes.
The distinguishing feature of the vegetative state is an irregular but cyclic state of circadian sleeping and waking unaccompanied by any behaviorally detectable expression of self-awareness, specific recognition of external stimuli, or consistent evidence of attention or intention or learned responses. Patients in a vegetative state are usually not immobile. They may move the trunk or limbs in meaningless ways. They may occasionally smile, and a few may even shed tears; some utter grunts or, on rare occasions, moan or scream. Some patients have acquired, nonhabitual startle myoclonus. Such activities are inconsistent, nonpurposeful, and coordinated only when they are expressed as part of a subcortical, instinctively patterned, reflexive response to external stimulation. These motor activities may misleadingly suggest purposeful movements, yet these responses have been observed in patients in whom careful study has disclosed no evidence of psychological awareness or the capacity to engage in learned behavior.
As a result of the relative preservation of brain-stem functions, most patients in a vegetative state retain good to normal reflexive regulation of vision and eye movement. Some patients have unequal or irregular pupils or limited responses to vestibulo-ocular stimulation. A few patients may have signs of mild internuclear ophthalmoplegia or other oculomotor abnormalities related to the brain stem. Occasionally, one or both third nerves are paralyzed.
Sustained visual pursuit is lacking in most patients in a vegetative state. They do not fixate on a visual target, track moving objects with their eyes, or withdraw from threatening gestures. When patients undergo a transition from the vegetative state to a state of awareness, one of the first and most readily observable signs of this transition is the appearance of sustained visual pursuit. However, patients in a vegetative state often have inconsistent primitive auditory or visual orienting reflexes, characterized by a turning of the head and eyes toward peripheral sounds or movements. In rare cases, patients who have no other evidence of consciousness over a period of months to years have some degree of briefly sustained visual pursuit or fixation, which is believed to be mediated through brain-stem structures. Nevertheless, one should be extremely cautious in making a diagnosis of the vegetative state when there is any degree of sustained visual pursuit, consistent and reproducible visual fixation, or response to threatening gestures.
The capacity for survival in a persistent vegetative state requires preservation of hypothalamic and brain-stem autonomic functions. Most patients who survive for a long time maintain normal body temperature, the ability to breathe spontaneously, and a functioning cardiovascular system. The prognosis is worse if there are hypothalamic disturbances producing central fever, excess sweating, disturbances in salt and water metabolism, and refractory pulmonary problems. In most patients, the gag, cough, sucking, and swallowing reflexes are preserved. Except for a lack of coordination in chewing and swallowing, gastrointestinal function remains nearly normal. As the prolonged survival of some patients in a persistent vegetative state suggests, autonomic function is sufficient to maintain long-term internal regulation so long as external needs receive constant attention.
Related Terms and Conditions
Unconsciousness, Coma, and the Vegetative State
The term "consciousness" was defined by William James in 1890 as awareness of the self and the environment. Consciousness has two dimensions: wakefulness and awareness. Normal consciousness requires arousal, an independent, autonomic-vegetative brain function subserved by ascending stimuli from the pontine tegmentum, posterior hypothalamus, and thalamus that activate wakefulness. Awareness is subserved by cerebral cortical neurons and their reciprocal projections to and from the major subcortical nuclei. Awareness requires wakefulness, but wakefulness can be present without awareness.
Unconsciousness implies global or total unawareness and is characteristic of both coma and the vegetative state. Patients in a coma are unconscious because they lack both wakefulness and awareness. Patients in a vegetative state are unconscious because, although they are wakeful, they lack awareness. In this report we use the terms awareness and consciousness interchangeably.
Persistent as Compared with Permanent Vegetative States
As originally defined by Jennett and Plum in 1972, the term "persistent," when applied to the vegetative state, meant sustained over time; "permanent" meant irreversible1. Notwithstanding Jennett and Plum's precise use of language, confusion has arisen over the exact meaning of the term "persistent." The adjective "persistent" refers only to a condition of past and continuing disability with an uncertain future, whereas "permanent" implies irreversibility. Persistent vegetative state is a diagnosis; permanent vegetative state is a prognosis.
A wakeful unconscious state that lasts longer than a few weeks is referred to as a persistent vegetative state. We define such a state operationally as a vegetative state present one month after an acute traumatic or nontraumatic brain injury or a vegetative state of at least one month's duration in patients with degenerative or metabolic disorders or developmental malformations. A permanent vegetative state, on the other hand, means an irreversible state, which like all clinical diagnoses in medicine, is based on probabilities, not absolutes. A patient in a persistent vegetative state becomes permanently vegetative when the diagnosis of irreversibility can be established with a high degree of clinical certainty -- that is, when the chance that the patient will regain consciousness is exceedingly small. We believe there are sufficient data on the prognosis for neurologic recovery to allow us to distinguish between persistent and permanent vegetative states. These data, in conjunction with other relevant factors in an individual patient, can be used by a physician to determine when the persistent vegetative state becomes permanent -- that is, when a physician can tell the patient's family or surrogate with a high degree of medical certainty that there is no further hope for recovery of consciousness or that, if consciousness were recovered, the patient would be left severely disabled.
Diagnostic Factors and the Limits of Certainty
By definition, patients in a persistent vegetative state are unaware of themselves or their environment. They are noncognitive, nonsentient, and incapable of conscious experience. There is, however, a biologic limitation to the certainty of this definition, since we can only infer the presence or absence of conscious experience in another person21. A false positive diagnosis of a persistent vegetative state could occur if it was concluded that a person lacked awareness when, in fact, he or she was aware. Such an error might occur if a patient in a locked-in state (i.e., conscious yet unable to communicate because of severe paralysis) was wrongly judged to be unaware. Thus, it is theoretically possible that a patient who appears to be in a persistent vegetative state retains awareness but shows no evidence of it. In the practice of neurology, this possibility is sufficiently rare that it does not interfere with a clinical diagnosis carefully established by experts.
Ave. S.E., Minneapolis, MN 55414.
References
|
|
|
|
|
|
|
|
|
|
|
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 1990