|
|
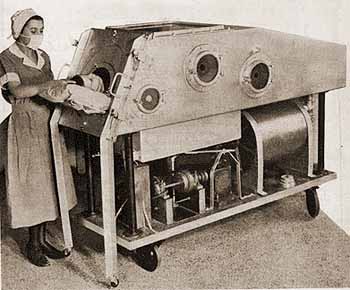
1937 “iron lung” |
|
|
1937 “iron lung” |
CARDIO
-
PULMONARY
RESUSCITATION (CPR)
MOUTH-to-MOUTH
RESUSCITATION
HIST: http://www.lifesaving.com/issues/articles/10evolution.html
Ancient
methods of resuscitation included:
(1) the application of heat, excrement or ashes;
(2) flagellation
|
|
|
|
More recent methods include:
16th century: blowing hot air and smoke into the victim's lungs with a bellows
|
|
|
|
|
18th
century:
(1) instilling smoke into the rectum;
(2) “inversion” (hanging drowning victims
upside-down);
(3) rolling victims over a barrel.
(3) placing victim on trotting horse.
19th
century:
(1) rolling victims 16 times per minute from
side-to-back,
applying pressure to the back
while prone;
(2) stretching the tongue
Modern CPR developed in the late 1950s and early 1960s. Dr. James O. Elam (1954) demonstrated the superiority of expired air ventilation without equipment over manual chest pressure; his work was confirmed during the next four years by Dr. Peter Safar. The American Red Cross mounted a campaign to teach mouth-to-mouth resuscitation for drowning victims.
CHEST
COMPRESSIONS
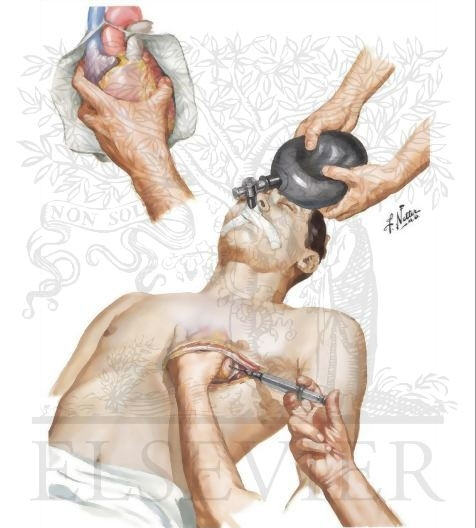
FROM 1950-1960 direct cardiac compression by squeezing the heart by hand through a hole cut in the left side of the victim's chest. The success rate was very low.
|
|
|
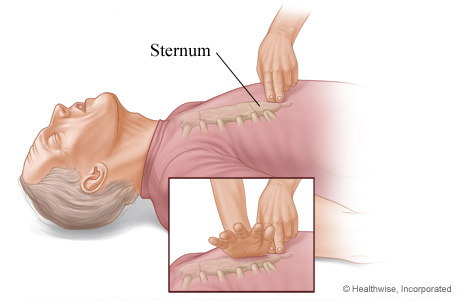
| internal cardiac massage | External Chest Compression |
In early 1960 Drs. Kouwenhoven, Knickerbocker, and Jude discovered the benefit of chest compression to achieve a small amount of artifical circulation. Later in 1960, mouth-to-mouth and chest compression were combined to create CPR as it is practiced today.
|
|
| Locate and avoid the Xyphoid Process |
RESPIRATORS
IN 1928, Philip Drinker and Louis Shaw at Harvard Medical School introduced the “iron lung” to help individuals suffering from acute poliomyelitis.
|
|
|
Polio impaired patients' ability to breathe by paralyzing the diaphragm and intercostal muscles; the iron lung provided relief in the form of artificial respiration.
 |
 |
 |
| 1955 Infant “iron lung” | Child in “iron lung” | Modern Respirator |
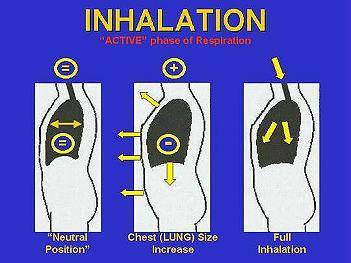
IT consisted of a sealed chamber in which air pressure is alternately reduced and increased. The patient was placed in the chamber with his/her head emerging from a port at one end. Each cycle of vacuum within the chamber allowed their lungs to be filled with atmospheric air; subsequent increase of pressure forced exhalation of air from the lungs.
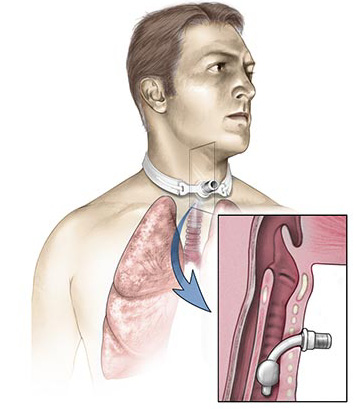
MODERN respirators provide “positive-pressure breathing” through a tube placed down the trachea
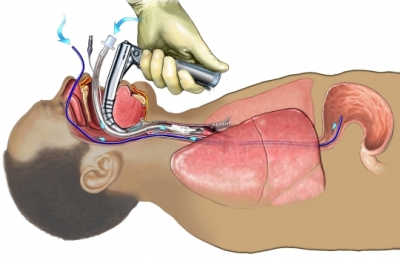 |
 |
or inserted through a hole in the next leading into the trachea.
 |
 |
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 1990