|
|
Articella, Medieval illum.MS |
|
|
Articella, Medieval illum.MS |
The Substance-Related disorders
encompass
10 separate classes of drugs:
|
[1] alcohol; [2] caffeine; [3] cannabis (marijuana); [4] hallucinogens (with separate categories for phencyclidine [or similarly acting arylcyclo-hexylamines] and other hallucinogens); [5] inhalants; |
[6] opioids; [7] sedatives, hypnotics, and anxiolytics; [8] stimulants (amphetamine-type substances, cocaine, and other stimulants); [9] tobacco; [10] and other (or unknown) substances. |
[1] SEDATIVE/ HYPNOTIC (DEPRESSANTS)
[1a] ALCOHOL (Ethanol)
There is no single, universal treatment for alcohol abuse. Initial treatment must take into account withdrawal symptoms, which can be serious and even fatal (see below), Subsequent treatment can involve drugs, psychotherapy (individual or group) and long-term strategies combining any or all of these.
Currently, three drugs are approved in the United States for treatment of alcoholism: disulfiram (ANTABUSE), has a long history of use but has fallen into disfavor because of its side effects and problems with patient adherence to therapy. When alcohol is ingested by a person who has taken disulfiram the result is headache, breathing difficulties, nausea and copious vomiting from acetaldehyde poisoning/
Naltrexone and acamprosate were introduced more recently. The goal of these medications is to assist the patient in maintaining abstinence. naltrexone (REVIA), decreases the urge to drink and causes mild nausea (especially in men) when alcohol is ingested. (Goodman and Gilman, 602-604)
TREATMENT LOCATIONS
Inpatient
Inpatient settings include medical detox and stabilization, dual-diagnosis hospital inpatient, and some therapeutic communities and residential programs (Perez, 2001; Stevens & Smith, 2013). These settings are often quite effective in helping clients with severe alcohol problems achieve abstinence, even out, and begin the process of therapy. They include medical services, individual counseling, group counseling, 12-step mutual support groups, religious services, meals, and shelter. Unfortunately, inpatient treatment stays are temporary, and thus many hospital centers experience the revolving door phenomenon, in which clients are treated for acute alcoholism but then return a few weeks later. These experiences necessitate the need for proper referral to less restrictive environments once clients are stabilized.
Outpatient
Outpatient-type settings include partial hospitalization and day treatment, temporary recovery or halfway homes, and outpatient or intensive outpatient treatment (Perez, 2001; Stevens & Smith, 2013). These settings allow the client to carry on with some or all aspects of his or her normal, day-to-day life. For example, in a day treatment center, the client needs to attend treatment during the day but is free to spend time with his or her family at home in the evenings. Outpatient settings are an essential follow-up for clients who matriculated through an inpatient or residential alcohol program. Among other interventions, relapse prevention strategies become important at this stage and setting of treatment. Traditional outpatient counseling is once a week, although intensive outpatient, partial hospitalization, and day treatment programs might include several group and individual sessions a week.
Physical dependence is demonstrated by the elicitation of a withdrawal syndrome when alcohol consumption is terminated. The symptoms and severity are determined by the amount and duration of alcohol consumption and include[:]
sleep disruption,
autonomic nervous system (sympathetic) activation,
tremors,
and in severe cases, seizures.
In addition, two or more days after withdrawal, some individuals experience delirium tremens, characterized by[:]
hallucinations,
delirium,
fever, and
tachycardia/
Delirium tremens can be fatal. Another aspect of dependence is craving and drug-seeking behavior, often termed psychological dependence.
[1b]
OPIOIDS (Narcotics: Opium-derivatives)
Morphine, Codeine, Oxycodone, Methadone, Heroin
[Goodman and Gilman 619] As with other addictions, the first stage of treatment addresses physical dependence and consists of detoxification (Kosten and O’Conner, 2003). The opioid-withdrawal syndrome (Table 24–7) is very unpleasant but not life-threatening. It begins within 6-12 hours after the last dose of a short-acting opioid and as long as 72-84 hours after a very long-acting opioid medication. Heroin addicts go through early stages of this syndrome frequently when heroin is scarce or expensive. Some therapeutic communities as a matter of policy elect not to treat withdrawal so that the addict can experience the suffering while being given group support. The duration and intensity of the syndrome are related to the clearance of the individual drug. Heroin withdrawal is brief (5-10 days) and intense. Methadone withdrawal is slower in onset and lasts longer. Protracted withdrawal also is likely to be longer with methadone. (See more detailed discussions of protracted withdrawal under “Long-Term Management” later in the chapter.)
[1c]
BARBITURATES
Phenobarbitol, Seconal
Treatment of abuse and addiction should be handled similarly to interventions for the abuse of alcohol and benzodiazepines. Because drugs in this category frequently are prescribed as hypnotics for patients complaining of insomnia, physicians should be aware of the problems that can develop when the hypnotic agent is withdrawn. Insomnia rarely should be treated with medication as a primary disorder except when produced by short-term stressful situations. Insomnia often is a symptom of an underlying chronic problem, such as depression or respiratory dysfunction, or may be due simply to a change in sleep requirements with age. Prescription of sedative medications, however, can change the physiology of sleep with subsequent tolerance to these medication effects. When the sedative is stopped, there is a rebound effect with worsened insomnia. This medication-induced insomnia requires detoxification by gradual dose reduction.
[2] ANTI-ANXIETY
[2a] BENZODIAZEPINES
Xanax, Valium, Librium,
[Goodman and Gilman 613-615]
Following moderate dose usage
Anxiety, agitation
Increased sensitivity to light and sound
Paresthesias, strange sensations
Muscle cramps
Myoclonic jerks
Sleep disturbance
Dizziness
Following high-dose usage
Seizures
Delirium
Deliberate abusers of high doses of benzodiazepines usually require inpatient
detoxification. Frequently, benzodiazepine abuse is part of a combined
dependence involving alcohol, opioids, and cocaine. Detoxification can be a
complex clinical pharmacological problem requiring knowledge of the
pharmacokinetics of each drug. The patient’s history may be unreliable not
simply because of lying but also because the patient frequently does not know
the true iden¬tity of drugs purchased on the street. Medication for
detoxification should not be prescribed by the “cookbook” approach but by
care¬ful titration and patient observation. The withdrawal syndrome from
diazepam, for example, may not become evident until the patient develops a
seizure in the second week of hospitalization. One approach to complex
detoxification is to focus on the CNS-depressant drug and temporarily hold the
opioid component con¬stant with a low dose of methadone. Opioid detoxification
can begin later. A long-acting benzodiazepine such as diazepam or clor-azepate (TRANXENE)
or a long-acting barbiturate such as phenobar¬bital can be used to block the
sedative withdrawal symptoms. The phenobarbital dose should be determined by a
series of test doses and subsequent observations to determine the level of
tolerance. Most complex detoxifications can be accomplished using this
phe¬nobarbital loading-dose strategy (see Robinson et al., 1981).
After detoxification, the prevention of relapse requires a long¬term outpatient
rehabilitation program similar to the treatment of alcoholism. No specific
medications have been found to be useful in the rehabilitation of sedative
abusers, but, of course, specific psychi¬atric disorders such as depression or
schizophrenia, if present, require appropriate medications.
[2b]
CANNABIS / THC
Marijuana
[3] STIMULANTS
[3a] COCAINE
[3b] AMPHETAMINES
Dexamphetamine, Ritalin
[3c] NICOTINE / TOBACCO
cigarettes, cigars, “The Patch” vaping
A combination of behavioral treatment with nicotine replacement to ease withdrawal and an anti-craving medication to reduce relapse is currently considered the treatment of choice.
[3d] CAFFEINE
Coffee, Tea, Chocolate, Soft Drinks
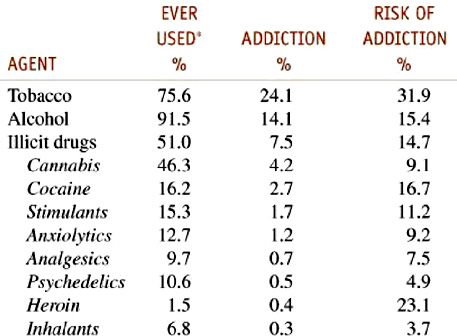
Table 24–2 Dependence among Users 1990–1992
Goodman and Gilman 2012 - Drug Addiction
Statistics from 1990-1994
|
|
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002