|
|
|
|
|
|
Cocaine / Amphetamines / Nicotine / Caffeine
AS the name suggests, stimulants increase alertness, attention, and energy, as well as elevate blood pressure, heart rate, and respiration. Stimulants historically were used to treat asthma and other respiratory problems, obesity, neurological disorders, and a variety of other ailments. But as their potential for abuse and addiction became apparent, the medical use of stimulants began to wane. Now, stimulants are prescribed to treat only a few health conditions, including ADHD (attention deficit hyperactivity disorder), narcolepsy, and occasionally depression—in those who have not responded to other treatments.
From the NIH Website: https://www.drugabuse.gov/publications/research-reports/prescription-drugs/stimulants/what-are-stimulants
|
|
Coca - Erythroxylum novogranatense |
COCAINE |
AFTER cannabis, cocaine is the most frequently used illegal drug globally. Between 14 and 21 million people use the drug each year. Used for thousands of years by the inhabitants of South America, it was imported into Europe in the 16th century. The active principle, cocaine, was identified by Friedrich Gaedcke in 1855.
More than 23 million Americans are estimated to have used cocaine at some time, but the number of current users declined from an estimated 8.6 million occasional users and 5.8 million regular users to 3.6 million who are currently estimated to be chronic cocaine users. The number of frequent users (at least weekly) has remained steady since 1991 at about 640,000. Not all users become addicts, [...] A key factor is the widespread availability of relatively inexpensive cocaine in the alkaloidal form (free base, “crack”) suitable for smoking and the hydrochloride powder form suitable for nasal or intravenous use. Drug abuse in men occurs about twice as frequently as in women. However, smoked cocaine use is particularly common in young women of childbearing age, who may use cocaine in this manner as commonly as do men. The reinforcing effects of cocaine and cocaine analogs correlate best with their effectiveness in blocking the transporter that recovers dopamine from the synapse. This leads to increased dopamine concentrations at critical brain sites (Ritz et al., 1987). However, cocaine also blocks both norepinephrine (NE) and serotonin (5-HT) reuptake, and chronic use of cocaine produces changes in these neurotransmitter systems, as measured by reductions in the neurotransmitter metabolites 3-methoxy-4 hydroxyphenethyleneglycol (MOPEG or MHPG) and 5- hydroxyindoleacetic acid (5-HIAA). [...]
Cocaine produces a dose-dependent increase in heart rate and blood pressure accompanied by increased arousal, improved performance on tasks of vigilance and alertness, and a sense of self-confidence and wellbeing. Higher doses produce euphoria, which has a brief duration and often is followed by a desire for more drug. Involuntary motor activity, stereotyped behavior, and paranoia may occur after repeated doses. Irritability and increased risk of violence are found among heavy chronic users. The half-life of cocaine in plasma is about 50 minutes, but inhalant (crack) users typically desire more cocaine after 10 to 30 minutes. Intranasal and intravenous uses also result in a high of shorter duration than would be predicted by plasma cocaine levels, suggesting that a declining plasma concentration is associated with termination of the high and resumption of cocaine seeking. This theory is supported by positronemission tomographic imaging studies using 11C-labeled cocaine, which show that the time course of subjective euphoria parallels the uptake and displacement of the drug in the corpus striatum (Volkow et al., 1999).
The major route for cocaine metabolism involves hydrolysis of each of its two ester groups. Benzoylecgonine, produced on loss of the methyl group, represents the major urinary metabolite and can be found in the urine for 2 to 5 days after a binge. As a result, benzoylecgonine tests are useful for detecting cocaine use; heavy users have detectable amounts of the metabolite in their urine for up to 10 days following a binge. Cocaine frequently is used in combination with other drugs such as heroin. [...] Alcohol is another drug that cocaine users take to reduce the irritability experienced during heavy cocaine use. Some develop alcohol addiction in addition to their cocaine problem. An important metabolic interaction occurs when cocaine and alcohol are taken concurrently. Some cocaine is transesterified to cocaethylene, which is equipotent to cocaine in blocking dopamine reuptake (Hearn et al., 1991).
Addiction is the most common complication of cocaine use. Some users, especially intranasal users, can continue intermittent use for years. Others become compulsive users despite elaborate methods to maintain control. Stimulants tend to be used much more irregularly than opioids, nicotine, and alcohol. Binge use is very common, and a binge may last hours to days, terminating only when supplies of the drug are exhausted.
Toxicity. Other risks of cocaine use, beyond the potential for addiction, involve cardiac arrhythmias, myocardial ischemia, myocarditis, aortic dissection, cerebral vasoconstriction, and seizures. reduce the irritability experienced during heavy cocaine use. Some develop alcohol addiction in addition to their cocaine problem. An important metabolic interaction occurs when cocaine and alcohol are taken concurrently. Some cocaine is transesterified to cocaethylene, which is equipotent to cocaine in blocking dopamine reuptake (Hearn et al., 1991).
Pregnant cocaine users may experience premature labor and abruptio placentae (Chasnoff et al., 1989). Attributing the developmental abnormalities reported in infants born to cocaine-using women simply to cocaine use is confounded by the infant’s prematurity, multiple-drug exposure, and overall poor pre- and postnatal care. Cocaine has been reported to produce a prolonged and intense orgasm if taken prior to intercourse, and its use is associated with compulsive and promiscuous sexual activity. Long-term cocaine use, however, usually results in reduced sexual drive; complaints of sexual problems are common among cocaine users presenting for treatment. Psychiatric disorders, including anxiety, depression, and psychosis, are common in cocaine users who request treatment. While some of these psychiatric disorders undoubtedly existed prior to the stimulant use, many develop during the course of the drug abuse (McLellan et al., 1979).
Tolerance, Dependence, and Withdrawal. Sensitization is a consistent finding in animal studies of cocaine and other stimulants. Sensitization is produced by intermittent use and typically is measured by behavioral hyperactivity. In human cocaine users, sensitization for the euphoric effect typically is not seen. On the contrary, most experienced users report requiring more cocaine over time to obtain euphoria, i.e., tolerance. In the laboratory, tachyphylaxis (rapid tolerance) has been observed with reduced effects when the same dose is given repeatedly in one session. Sensitization may involve conditioning (Figure 23–2). Cocaine users often report a strong response on seeing cocaine before it is administered, consisting of physiological arousal and increased drug craving with concomitant activation of brain limbic structures (Childress et al., 1999). Sensitization in human beings has been linked to paranoid, psychotic manifestations of cocaine use based on the observation that cocaine-induced hallucinations and paranoia typically are seen after long-term exposure (mean 35 months) in vulnerable users (Satel et al., 1991). Since cocaine typically is used intermittently, even heavy users go through frequent periods of withdrawal or “crash.” The symptoms of withdrawal seen in users admitted to hospitals are listed in Table 23–8. Careful studies of cocaine users during withdrawal show gradual diminution of these symptoms over 1 to 3 weeks (Weddington et al., 1990). Residual depression may be seen after cocaine withdrawal and should be treated e treated with antidepressant agents if it persists
Cocaine Withdrawal Symptoms and Signs
Dysphoria, depression
Sleepiness, fatigue
Cocaine craving
Bradycardia
Pharmacological Interventions. Since cocaine withdrawal is generally mild, treatment of withdrawal symptoms usually is not required. The major problem in treatment is not detoxification but helping the patient to resist the urge to restart compulsive cocaine use. Rehabilitation programs involving individual and group psychotherapy based on the principles of Alcoholics Anonymous and behavioral treatments based on reinforcing cocaine-free urine tests result in significant improvement in the majority of cocaine users (Alterman et al., 1994; Higgins et al., 1994). Nonetheless, there is great interest in finding a medication that can aid in the rehabilitation of cocaine addicts.
|
|
|
|
DISCOVERED in 1887, Lazar Edeleanu synthesized the drug at the University of Berlin. It was not used medicinally until the 1930s when it became widely available over the counter; and it was employed during World War II by the military in Germany, Japan, and the U.S. to increase the stamina of soldiers:
“Their official selling point was their beneficial action in relieving nasal congestion, the discomfort of a blocked nose. But they did more. They were soon recognised as stimulants, more powerful than cocaine and much cheaper. They reduced hunger and especially the comfort eating of the anxious and the worried. This made them weight-reducers. Most strikingly, they built up confidence and endurance. They were capable of enhancing performance even in such allegedly ‘unalterable’ markers as the standard IQ. (The snag was that the change could be in either direction, accounting for unexpected examination disasters as well as fantastic successes.) They would also reduce the impact of pain on morale. They tended to still ‘conventional’ doubts, scruples and misgivings. The last made them a boon to military commanders. As with aerial bombs and nerve gases, the Spanish Civil War provided the ideal testing ground. Amphetamines were lavishly doled out by both sides to overcome flagging morale and battle fatigue. They were politically impartial but may have prolonged the conflict by a few months.
But it was the Second World War which saw their potential fully used. Millions of metamphetamine tablets were distributed with the food rations to British, German, Italian and Japanese troops. From Britain most of the initially limited supply went to hard-pressed troops in Africa. It made the heat and the sand more bearable. Did it help to stop Rommel’s advance? Perhaps. But the drug also sustained morale on the Home Front, easing the suffering both of the bereaved and of those trapped under the rubble of collapsing buildings. A tablet or two helped to pass the night in crowded improvised air-raid shelters. In 1941 the Evening News carried the headline: `Methedrine wins the Battle of London'."
By 1943 Japanese production reached such a level that at the time of the country's surrender in 1945 an estimated hundred billion tablets were stashed in military warehouses. The stocks disappeared within weeks, flooding the streets first of Tokyo and then of cities in the United States with cheap capsules. They reached millions of delirious users, engendering an estimated 100,000 suicides. For some years they were thought to be partly at least responsible for half the murders in California and the same proportion of self-inflicted mental illnesses. Even by enthusiasts the last was recognised as a distinct drawback. Even small doses in those susceptible could cause delusions, megalomania and violent symptoms of persecution indistinguishable from schizophrenia. In some the mental illness persisted even after the drug was discontinued.
The post-war period shifted the pattern of users to lonely old people, tired housewives and despairing university students. Two pills are better than one month’s vacation; one advertisement ran. Dextroamphetamine was still advertised mainly as a painkiller. ‘Shrug off your discomforts! Shrug off your exhaustion! Shrug off your pain!’ It was probably in the mid-1950s that competitive sportsmen and women began to embrace it. In 1958 a champion cyclist died during a practice ascent in the French Alps fuelled by methedrine. A week later ten participants of the Tour de France fell sick with ‘acute amphetamine intoxication’. Two had to he admitted to a mental hospital to control their schizoid symptoms. The regulating bodies of international sport began to take note. Routine urine testing was beginning to be canvassed.” (The Worst of Evils, 414-417)
Subjective effects similar to those of cocaine are produced by amphetamine, ‘dextroamphetamine, methamphetamine, phenmetrazine, ‘methylphenidate, and diethylpropion.
Amphetamines ‘increase synaptic dopamine primarily by stimulating presynaptic release rather than by blockade of reuptake, as is the case with cocaine. Intravenous or smoked methamphetamine ‘produces an abuse/dependence syndrome similar ‘to that of cocaine, although clinical deterioration may ‘progress more rapidly. In animal studies, methamphetamine ‘in doses comparable with those used by human ‘abusers produces neurotoxic effects in dopamine and ‘serotonin neurons. Methamphetamine can be produced in ‘small, clandestine laboratories starting with ephedrine, a ‘widely available nonprescription stimulant.
Oral stimulants, ‘such as those prescribed in a weight-reduction program, have short-term efficacy because of tolerance development. Only a small proportion of patients introduced to these appetite suppressants subsequently exhibits dose escalation or drug seeking from various physicians; such patients may meet diagnostic criteria for abuse or addiction. Fenfluramine (no longer marketed in the United ‘States) and phenylpropanolamine (no longer marketed ‘in the United States) reduce appetite with no evidence of ‘significant abuse potential. Mazindol (no longer marketed ‘in the United States) also reduces appetite, with less stimulant ‘properties than amphetamine.
From the Wikipedia aricle on methamphetamine:
[Relatively easilysynthesized from available precursors . . .]
In low doses, methamphetamine can elevate mood, increase alertness, concentration and energy in fatigued individuals, reduce appetite and promote (initial) weight loss. At higher doses, it can induce
psychosis,
breakdown of skeletal muscle,
seizures and
bleeding in the brain.
Chronic high-dose use can precipitate
unpredictable and rapid mood swings,
prominent delusions and
violent behavior.
Recreationally, methamphetamine's ability to increase energy has been reported to lift mood and increase sexual desire to such an extent that users are able to engage in sexual activity continuously for several days.[17] Methamphetamine is known to have a high addiction liability (i.e. compulsive methamphetamine use) and dependence liability (i.e. withdrawal symptoms occur when methamphetamine use ceases). Heavy recreational use of methamphetamine may lead to a post-acute-withdrawal syndrome, which can persist for months beyond the typical withdrawal period.
Unlike amphetamine,
methamphetamine is neurotoxic to human midbrain dopaminergic neurons.[18]
It has also been shown to damage serotonin neurons in the CNS.[19][20]
This damage includes adverse changes in brain structure and function, such as reductions in grey matter volume in several brain regions and adverse changes in markers of metabolic integrity.[20]
17. San Francisco Meth Zombies (TV documentary). National Geographic Channel. August 2013. ASIN B00EHAOBAO.
18.
Malenka RC, Nestler EJ, Hyman SE (2009). "15". In Sydor A, Brown RY. Molecular
Neuropharmacology: A Foundation for Clinical Neuroscience (2nd
ed.). New York: McGraw-Hill Medical. p. 370. ISBN 978-0-07-148127-4. Unlike
cocaine and amphetamine, methamphetamine is directly toxic to midbrain
dopamine neurons.
19. Yu S, Zhu L, Shen Q, Bai X, Di X (2015). "Recent advances in methamphetamine neurotoxicity mechanisms and its molecular pathophysiology". Behav Neurol. 2015: 103969. doi:10.1155/2015/103969. PMC 4377385. PMID 25861156.
20.
Krasnova IN, Cadet JL
(May 2009). "Methamphetamine
toxicity and messengers of death". Brain
Res. Rev. 60 (2):
379–407. doi:10.1016/j.brainresrev.2009.03.002. PMC 2731235![]() . PMID 19328213.
. PMID 19328213. Neuroimaging
studies have revealed that METH can indeed cause neurodegenerative changes
in the brains of human addicts (Aron and Paulus, 2007; Chang et al., 2007).
These abnormalities include persistent decreases in the levels of dopamine
transporters (DAT) in the orbitofrontal cortex, dorsolateral prefrontal
cortex, and the caudate-putamen (McCann et al., 1998, 2008; Sekine et al.,
2003; Volkow et al., 2001a, 2001c). The density of serotonin transporters
(5-HTT) is also decreased in the midbrain, caudate, putamen, hypothalamus,
thalamus, the orbitofrontal, temporal, and cingulate cortices of
METH-dependent individuals (Sekine et al., 2006) ... Neuropsychological
studies have detected deficits in attention, working memory, and
decision-making in chronic METH addicts ... There is compelling evidence
that the negative neuropsychiatric consequences of METH abuse are due, at
least in part, to drug-induced neuropathological changes in the brains of
these METH-exposed individuals ...
Structural magnetic resonance imaging
(MRI) studies in METH addicts have revealed substantial morphological
changes in their brains. These include loss of gray matter in the cingulate,
limbic and paralimbic cortices, significant shrinkage of hippocampi, and
hypertrophy of white matter (Thompson et al., 2004). In addition, the brains
of METH abusers show evidence of hyperintensities in white matter (Bae et
al., 2006; Ernst et al., 2000), decreases in the neuronal marker, N-acetylaspartate
(Ernst et al., 2000; Sung et al., 2007), reductions in a marker of metabolic
integrity, creatine (Sekine et al., 2002) and increases in a marker of glial
activation, myoinositol (Chang et al., 2002; Ernst et al., 2000; Sung et
al., 2007; Yen et al., 1994). Elevated choline levels, which are indicative
of increased cellular membrane synthesis and turnover are also evident in
the frontal gray matter of METH abusers (Ernst et al., 2000; Salo et al.,
2007; Taylor et al., 2007).
|
Nicoteana Tobanicum |
|
NICOTINE |
BECAUSE nicotine provides the reinforcement for cigarette smoking, the most common cause of preventable death and disease in the U.S., it is arguably the most dangerous dependence-producing drug. The dependence produced by nicotine can be extremely durable, as exemplified by the high failure rate among smokers who try to quit. Although >80% of smokers express a desire to quit, only 35% try to stop each year, and fewer than 5% are successful in unaided attempts to quit (American Psychiatric Association, 2000).
Nicotine is a naturally occurring alkaloid found in tobacco plants, a tightly woven skein of carbon, hydrogen, and nitrogen (C10H14N2). The tobacco plant, in fact, belongs to the rather notorious nightshade family, a group overpopulated with toxic vegetation, including mandrake, jimson weed, and deadly nightshade, from which the poison belladonna is produced. Nicotine had been isolated and synthesized in the nineteenth century. In pure form, it took an ounce at most to kill the average adult.[...]
DEADLY carbon monoxide is also produced by burning tobacco. In 1933 “ [...] [carbon monoxide [carboxyhemoglobin] blood levels for country dwellers averaged less than 1 percent saturation. The levels for Manhattan street cleaners (who inhaled high doses of automobile exhaust) were triple that amount, a solid 3 percent. But smokers came in the highest, higher than [the medical examiner] expected [...]: Americans were inhaling a lot more tobacco smoke than they had once done, and their saturation levels ranged from 8 to 19 percent.”
|
CARBON MONOXIDE |
HYDROGEN SULFIDE |
CYANIDE |
“Tobacco smoke contain[s] more than nicotine and carbon monoxide. It also contains cyanide, hydrogen sulfide, formaldehyde, ammonia, and pyridine, the latter a component in industrial solvents.” (The Poisoner's Handbook, Deborah Blum, 2011)
Cigarette (nicotine) addiction is influenced by multiple variables. Nicotine itself produces reinforcement; users compare nicotine to stimulants such as cocaine or amphetamine, although its effects are of lower magnitude. While there are many casual users of alcohol and cocaine, few individuals who smoke cigarettes smoke a small enough quantity (≤5 cigarettes per day) to avoid dependence. Nicotine is absorbed readily through the skin, mucous membranes, and lungs. The pulmonary route produces discernible CNS effects in as little as 7 seconds. Thus, each puff produces some discrete reinforcement. With 10 puffs per cigarette, the one-pack-per-day smoker reinforces the habit 200 times daily. The timing, setting, situation, and preparation all become associated repetitively with the effects of nicotine. Nicotine activates the nucleus accumbens reward system in the brain; increased extracellular DA has been found in this region after nicotine injections in rats. Nicotine affects other systems as well, including the release of endogenous opioids and glucocorticoids.
|
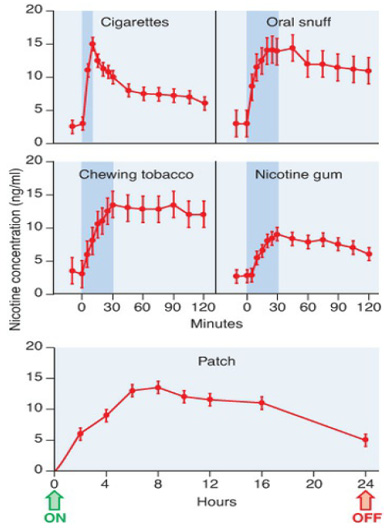
NICOTINE CONCENTRATIONS in BLOOD |
|
|
Figure 24–3. Nicotine concentrations in blood resulting from five different nicotine delivery systems. Shaded areas (upper panel) indicate the periods of exposure to nicotine. Arrows (lower panel) indicate when the nicotine patch was put on and taken off. (From Benowitz et al., 1988, and Srivastava et al, 1991, Benowitz et al, 1988.
There is evidence for tolerance to the subjective effects of nicotine. Smokers typically report that the first cigarette of the day after a night of abstinence gives the “best” feeling. Smokers who return to cigarettes after a period of abstinence may experience nausea if they return immediately to their previous dose. Persons naive to the effects of nicotine will experience nausea at low nicotine blood levels, and smokers will experience nausea if nicotine levels are raised above their accustomed levels.
Negative reinforcement refers to the benefits obtained from the termination of an unpleasant state. In dependent smokers, the urge to smoke correlates with a low blood nicotine level, as though smoking were a means to achieve a certain nicotine level and thus avoid withdrawal symptoms. Some smokers even awaken during the night to have a cigarette, which ameliorates the effect of low nicotine blood levels that could disrupt sleep. If the nicotine level is maintained artificially by a slow intravenous infusion, the number of cigarettes smoked and in the number of puffs decrease. Thus, smokers may be smoking to achieve the reward of nicotine effects, to avoid the pain of nicotine withdrawal, or most likely a combination of the two. Nicotine withdrawal symptoms are listed here:
Nicotine Withdrawal Symptoms
|
Irritability, impatience, hostility Anxiety Dysphoric or depressed mood Difficulty concentrating Restlessness Decreased heart rate Increased appetite or weight gain |
Depressed mood (dysthymic disorder, affective disorder) is associated with nicotine dependence, but it is not known whether depression predisposes one to begin smoking or depression develops during the course of nicotine dependence. Depression increases significantly during smoking withdrawal, and this is cited as one reason for relapse.
Pharmacological Interventions. The nicotine withdrawal syndrome can be alleviated by nicotine-replacement therapy, available with a prescription (e.g., NICOTROL inhaler and nasal spray) or without (e.g., NICORETTE gum and others; COMMIT lozenges and others; and NICODERM CQ transdermal patch and others). shows the blood nicotine concentrations achieved by different methods of nicotine delivery. Because nicotine gum and a nicotine patch do not achieve the peak levels seen with cigarettes, they do not produce the same magnitude of subjective effects as smoking. These methods do, however, suppress the symptoms of nicotine withdrawal. Thus, smokers should be able to transfer their dependence to the alternative delivery system and gradually reduce the daily nicotine dose with minimal symptoms. Although this results in more smokers achieving abstinence, most resume smoking over the ensuing weeks or months. Comparisons with placebo treatment show large benefits of nicotine replacement at 6 weeks, but the effect diminishes with time. The nicotine patch produces a steady blood level and seems to have better patient compliance than that observed with nicotine gum. Verified abstinence rates at 12 months are reported to be in the range of 20%. The necessary goal of complete abstinence contributes to the poor success rate; when ex-smokers “slip” and begin smoking a little, they usually relapse quickly to their prior level of dependence.
The search for better medications to treat nicotine addiction has become an important goal of the pharmaceutical industry, and other types of medication have been tested in clinical trials. A sustained-release preparation of the antidepressant bupropion (ZYBAN; improves abstinence rates among smokers and remains a useful option. The cannabinoid CB1 receptor mechanism led to a high frequency of depressive and neurologic symptoms, ending its development in the U.S. Varenicline, a partial agonist at the α4β2 inverse agonist rimonabant improves abstinence rates and reduces the weight gain seen frequently in ex-smokers. Unfortunately, the CB1 inverse agonist subtype of the nicotinic acetylcholine receptor, improves abstinence rates but has also been linked to risk of developing suicidal ideation. Varenicline partially stimulates nicotinic receptors, thereby reducing craving and preventing most withdrawal symptoms. It has high receptor affinity, thus blocking access to nicotine, so if the treated smoker relapses, there is little reward and abstinence is more likely to be maintained. In one recent clinical trial, the abstinence rate for varenicline at 1 year was 36.7% versus 7.9% for placebo (Williams et al., 2007).
|
|
Coffee leaves and beans |
CAFFEINE, a mild stimulant, is the most widely used psychoactive drug in the world. It is present in soft drinks, coffee, tea, cocoa, chocolate, and numerous prescription and over-the-counter drugs.
|
|
|
|
CAFFEINE |
THEOBROMINE |
LEGENDS concerning the origins of coffee abound. According to one version an Ethiopian goatherd noticed that after eating the berries from a certain tree, his goats became so energetic that they did not want to sleep at night. He reported this to the abbot of the local monastery, who compared the alertness of the goats with that of his monks during the night office. The Abbot made a drink with the berries and found that it kept his community alert through the long hours of nocturnal prayer. The abbot shared his discovery with the other monks at the monastery, and knowledge of the energizing berries began to spread. At one point - again according to legend - the concoction was found to be so effective that it was banned as heretical.
Caffeine mildly increases norepinephrine and dopamine release and enhances neural activity in numerous brain areas. Caffeine is absorbed from the digestive tract and is distributed rapidly throughout all tissues and easily crosses the placental barrier. Many of caffeine’s effects are believed to occur by means of competitive antagonism at adenosine receptors. Adenosine is a neuromodulator that influences a number of functions in the CNS . The mild sedating effects that occur when adenosine activates particular adenosine-receptor subtypes can be antagonized by caffeine.
Tolerance occurs rapidly to the stimulating effects of caffeine. Thus a mild withdrawal syndrome has been produced in controlled studies by abrupt cessation of as little as one to two cups of coffee per day.
Caffeine withdrawal consists of feelings of fatigue and sedation. With higher doses, headaches and nausea have been reported during withdrawal; vomiting is rare (Silverman et al., 1992). Although a withdrawal syndrome can be demonstrated, few caffeine users report loss of control of caffeine intake or significant difficulty in reducing or stopping caffeine, if desired (Dews et al., 1999). Thus, caffeine is not listed in the category of addicting stimulants (American Psychiatric Association, 1994).
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002