|
|
Articella, Medieval illum.MS |
|
|
Articella, Medieval illum.MS |
IT is important to be able to distinguish the different classes of drugs associated with addiction. Also important is an appreciation of the difference between dependency characterized by severe, even life-threatening withdrawal-symptoms (alcohol, opiates, cocaine), less intense withdrawal (nicotine/tobacco). and dependency characterized by milder withdrawal symptoms: (caffeine). The DSM5 lists ten classes of drugs associated with addiction (or substance-abuse disorder):
SUBSTANCE-RELATED
and ADDICTIVE
DISORDERS
DSM-5 pp. 481-591
The Substance-Related disorders
encompass
10 separate classes of drugs:
|
[1] alcohol; [2] caffeine; [3] cannabis (marijuana); [4] hallucinogens (with separate categories for phencyclidine [or similarly acting arylcyclo-hexylamines] and other hallucinogens); [5] inhalants;
|
[6] opioids; [7] sedatives, hypnotics, and anxiolytics; [8] stimulants (amphetamine-type substances, cocaine, and other stimulants); [9] tobacco; [10] and other (or unknown) substances. |
THESE 10 classes are not fully distinct. All drugs that are taken in excess have in common direct activation of the brain reward system, which is involved in the reinforcement of behaviors and the production of memories. They produce such an intense activation of the reward system that normal activities may be neglected. Instead of achieving reward system activation through adaptive behaviors, drugs of abuse directly activate the reward pathways.
THE pharmacological mechanisms by which each class of drugs produces reward are different, but the drugs typically activate the system and produce feelings of pleasure, often referred to as a “high.” Furthermore, individuals with lower levels of self-control, which may reflect impairments of brain inhibitory mechanisms, may be particularly predisposed to develop substance use disorders, suggesting that the roots of substance use disorders for some persons can be seen in behaviors long before the onset of actual substance use itself.
[1] SEDATIVE/ HYPNOTIC (DEPRESSANTS)
[1a] ALCOHOL (Ethanol)
[1b]
OPIOIDS (Narcotics: Opium-derivatives)
Morphine, Codeine, Oxycodone, Methadone, Heroin
[1c]
BARBITURATES
Phenobarbitol, Seconal
[2] ANTI-ANXIETY
[2a] BENZODIAZEPINES
Xanax, Valium, Librium,
Dependence and Tolerance occur. Withdrawal: rebound anxiety [65% of short-term users]; malaise, weakness, insomnia, rapid heart rate, lightheadedness, and dizziness; rarely seizures.
[2b]
CANNABIS / THC
Marijuana
[3] STIMULANTS
[3a] COCAINE
[3b] AMPHETAMINES
Dexamphetamine, Ritalin
[3c] NICOTINE / TOBACCO
cigarettes, cigars, “The Patch” vaping
[3d] CAFFEINE
Coffee, Tea, Chocolate, Soft Drinks
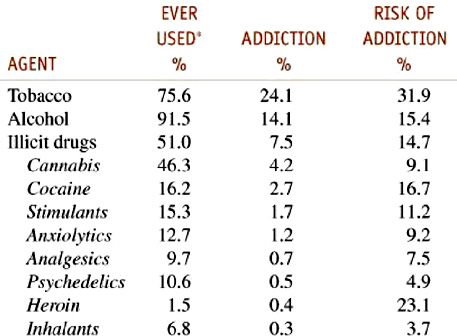
Table 24–2 Dependence among Users 1990–1992
Goodman and Gilman 2012 - Drug Addiction
Statistics from 1990-1994
|
|
America dulls its
pain and shortens life spans:
Another largely unremarked crisis: opiates.
Marcus Roberts | Mar 13 2017 |
https://www.mercatornet.com/demography/view/another-largely-unremarked-crisis-in-the-usa/19470
The current scale of the current spate of heroin/opioid abuse is unprecedented. In 2015, 52,000 Americans died of overdoses, four times the gun homicide rate and 50 per cent more than died in car accidents. In Rhode Island, 2 per cent of the population (20,000 people) are estimated by one epidemiologist to be opioid addicts. In Salisbury, Massachusetts (population 8,000) there have been 15 heroin overdoses in the last two years (it lost one person throughout the entire Vietnam War). In Huntington, West Virginia there were 28 overdoses in four hours last summer (out of a population of 49,000). These sorts of statistics have played a role in the decline in US life expectancy in 2015. Caldwell argues that it was not wrong for President Trump to describe the drug epidemic in his inaugural address as “carnage”.
Caldwell charts the way that the American tolerance for opiates has changed over time – they were over prescribed after the Civil War until the early part of last century, then were banned and taboo during the twentieth century. In the last twenty years, however, the taboo has been lifted due to libertine attitudes about drugs and a “massive corporate marketing effort”. For drug companies opioids were lucrative opportunities. Thus,
“In 1996, Purdue Pharmaceuticals brought to market OxyContin, an “extended release” version of the opioid oxycodone. (The “-contin” suffix comes from “continuous.”) The time-release formula meant companies could pack lots of oxycodone into one pill, with less risk of abuse, or so scientists claimed. Purdue did not reckon with the ingenuity of addicts, who by smashing or chewing or dissolving the pills could release the whole narcotic load at once. That is the charitable account of what happened. In 2007, three of Purdue’s executives pled guilty to felony misbranding at the time of the release of OxyContin, and the company paid $600 million in fines. In 2010, Purdue brought out a reformulated OxyContin that was harder to tamper with. Most of Purdue’s revenues still come from OxyContin. In 2015, the Sackler family, the company’s sole owners, suddenly appeared at number sixteen on Forbes magazine’s list of America’s richest families.”
The relaxation of taboos and a ready supply created a wider appetite for opioids. And for many people seeking an opioid hit, heroin turned out to be cheaper and easier to get. Its price declined in the last decade, its purity increased and the number of heroin deaths has also increased. Indeed, one opioid (fentanyl) is so lethal and starting to replace so much heroin, that in Maryland the number of fentanyl deaths in the first six months of 2016 increased nearly 400% (to 446) from the same period the year before. No wonder that the US life expectancy is decreasing!
To put the current epidemic of deaths into perspective,
the Nixon White House panicked when heroin-addicted soldiers back from Vietnam brought the overdose death rate to 1.5 per 100,000 in 1973-1975.
The crack epidemic of the mid to late 1980s reached a death rate of 2 per 100,000 and George H. W. Bush declared war on drugs.
[2016] The current opioid death rate is 10.3 per 100,000 without the fentanyl statistics of 2016
In New Hampshire the rate is 30 per 100,000
and in West Virginia it is over 40 per 100,000.
[2020] 28.3 per 100,000
[2021] 32.4 per 100,000*
*https://www.cdc.gov/drugoverdose/deaths/index.html#:~:text=Opioids%E2%80%94mainly%20synthetic%20opioids%20(other,of%20all%20drug%20overdose%20deaths).
This is a large reason why the life expectancy of middle-aged white people is falling. Why Bill Clinton said during last year’s campaign that poor white people were dying of “a broken heart” and why heroin is “a symbol of both working-class depravity and ruling-class neglect—an explosive combination in today’s political climate”.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2002