|
|
Jacob's Ladder: Medieval illum.MS |
|
|
Jacob's Ladder: Medieval illum.MS |
THE so-called “Transtheoretical” or “Stages-of-Change” model was first proposed by James O. Prochaska in 1977 and has been subsequently modified by him and others. It posits movement through a series of stages leading to behavioral change. Different forms of the model have been proposed, depending chiefly on whether relapse is incorporated into the model or regarded as an intermittent variation. It is sometimes depicted as a stairway or cycle, sometimes as a recurring helix
A ROUGH description of the stages would include:
· Precontemplation (Not Ready) – “People are not intending to take action in the foreseeable future, and can be unaware that their behaviour is problematic”
· Contemplation (Getting Ready) – “People are beginning to recognize that their behaviour is problematic, and start to look at the pros and cons of their continued actions”
· Preparation (Ready) – “People are intending to take action in the immediate future, and may begin taking small steps toward behaviour change”
· Action – “People have made specific overt modifications in modifying their problem behaviour or in acquiring new healthy behaviours”
· Maintenance – “People have been able to sustain action for at least six months and are working to prevent relapse”
[· Relapse – Individuals may fall out of the stages and re-enter at any point, unuslly pre-contemplation]
[· Termination – “Individuals have zero temptation and they are sure they will not return to their old unhealthy habit as a way of coping”]
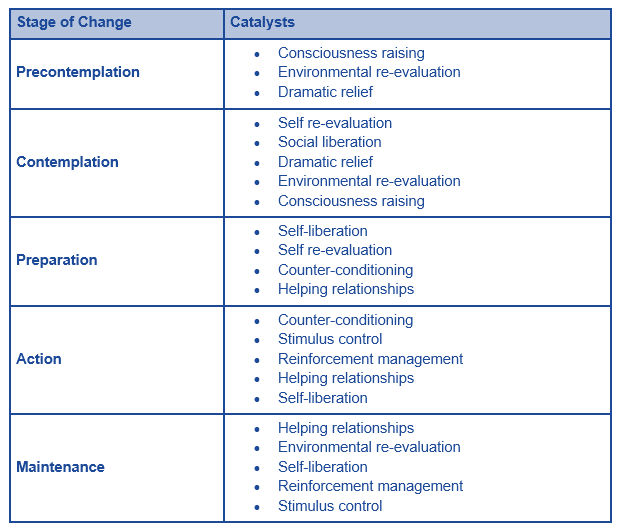
A MORE detailed description of the stages is provided by D.L. Thombs, Introduction to Addictive Behaviors, Chapter 10, “Conditions That Facilitate and Inhibit Change in Addictive Behavior” The Guilford Substance Abuse Series, (The Guilford Press, NY, 2006), 254-258
STAGES of CHANGE in ADDICTIVE BEHAVIOR
Motivation is a particularly critical issue in helping clients (or even communities) to change. Prochaska et al. (1992) developed a transtheoretical, stage model to explain how individuals change unwanted behavior as well as maintain new habits. The stages-of-change model is not another theory but a framework that can organize existing theories to help explain the process people use to change themselves—with or without professional assistance. Within each stage, constructs from various theories can be used to explain movement. It is important to note that the model does not explain why people change but, rather, how they do so.
Practitioners and researchers have shown much interest in the model because it provides a structure for understanding readiness to change problem behavior. The model has been applied to a variety of health behavior problems characterized by relapse. These have included medication adherence in AIDS treatment (Bradley-Springer, 1996), smoking cessation (DiClemente et al., 1991), recovery from alcohol/drug addiction (DiClemente, 1991), weight control (Prochaska & DiClemente, 1985), and psychological distress (Prochaska & Norcross, 1983).
Research has shown that the stages-of-change model is particularly useful for matching patients with treatments based on their readiness for change. Prochaska and DiClemente (1992) noted that many psychosocial and medical treatment programs have poor outcomes because they assume that new clients (or patients) are highly motivated to participate in their own treatment. In reality, across a broad range of behavioral and medical disorders, clients often do not possess a high level of readiness for change at the onset of treatment. Prochaska and DiClemente (1992) estimated that across populations with active health problems, roughly 10–15% are prepared to take action to improve their condition upon entering treatment.
The stages-of-change model consists of five stages (Prochaska & DiClemente, 1992). Each stage and its implications for helping individuals with substance-abusing problems are described here. It is important to point out that progression through these stages does not usually occur in a linear fashion. Clients who reach the latter three stages often recycle to the first two. However, research does indicate that for most individuals, relapsing is not an endless process (Prochaska & DiClemente, 1992). Most of the time, individuals do not regress all the way back to where they began. It appears that many learn from their mistakes and relapses become less frequent over time.
Precontemplation
Precontemplation describes a stage in which there is no intention to change behavior in the foreseeable future. Often, precontemplators do not define the behavior as a problem (DiClemente, 1991). Bell and Rollnick (1996) described them as “happy users.” However, external observers such as their friends, families, employers, and so on identify their behavior as problematic.
[1] DiClemente (1991) argued that there is more to precontemplation than just “denial” and “resistance.” Some precontemplators simply lack knowledge about the risks associated with their behavior.
[2] Others are rebellious because they have a heavy investment in maintaining the problem behavior.
[3] On the other hand, some precontemplators are characterized by resignation. They are overwhelmed by the problem and see themselves as incapable of change; they have no hope and believe it is too late to modify their behavior.
[4] Finally, some precontemplators involve themselves in rationalizing away the problem (e.g., “what’s the use of going through all the hassle of treatment, you only live once”).
DiClemente (1991) argued that there is a pervasive myth in the helping professions pertaining to precontemplators. The myth maintains that the more serious the health or behavior problem, the more intense the education, treatment, or confrontation must be to help the person. With precontemplators, “more” help may actually be harmful or, more commonly, just ignored. Research on brief interventions indicate that they are as effective as more intensive treatment and more effective than no treatment (Miller & Rollnick, 2002; NIAAA, 1997; Bernstein et al., 2005). This may be particularly the case when the focus of the brief intervention is to motivate the client to make a commitment to change.
Contemplation
Contemplation is a stage at which many substance abusers stay for an extended period. Typically, this stage involves an extended “risk–reward analysis” (DiClemente, 1991). Patients are involved in the frequent weighing of the costs and benefits of change. They mull over cost and benefits again and again. In contrast to the precontemplator, the contemplator is willing to consider change, but his/her ambivalence often makes this state chronic. For instance, DiClemente and Prochaska (1985) followed a group of 200 cigarette smokers in the contemplation stage for 2 years and found that the group’s modal or most common response was unchanged during this period.
Contemplators have an interest in change but little commitment. They demonstrate this by asking about treatment options but not following through, or by scheduling appointments only to fail to show up for them. DiClemente (1991) indicated that contemplators often offer reasons for why “now is not the right time” to begin a program (p. 195).
In working with contemplators, the challenge for practitioners is to facilitate movement toward the next stage: preparation.
The content of the information given to contemplators is important.
First, it should be personally relevant to the individual; a cocaine-dependent person considering treatment may not be swayed by information about Alcoholics Anonymous or long-term sobriety.
Second, there is a need to emphasize the benefits of change (e.g., “You can stop wasting money on crack), rather than attempting to arouse fear (e.g., “You’re damaging your heart and lungs,” or “You are going to end up in prison”). A focus on the benefits of change can create incentives for contemplator. Fear arousal messages (scare tactics) generally should be avoided because they serve to undermine self-efficacy; that is, they destroy optimism about the prospects for change by implying “it may already be too late for me.”
Preparation (or Determination)
In the preparation stage, persons form an intention to change a behavior in the near future (Prochaska & DiClemente, 1992). Their determination is often demonstrated by small behavior changes. People are typically in this stage for only brief periods. Their experimenting does not necessarily propel them into the next stage: action (DiClemente, 1991). Experiencing barriers to change may result in a return to contemplation.
DiClemente (1991) noted that an important task in helping the client in preparation is to encourage the development of a realistic plan of action. Many determined clients fail to recognize or dismiss the difficulties they will encounter when they take action (e.g., entering treatment). A realistic plan will anticipate these barriers and have identified solutions or responses for them.
Action
The next stage, action, involves implementing a plan. Here, people modify their behavior and/or their environment to overcome a problem. However, as Prochaska and DiClemente (1992) noted:
Modifications of the addictive behavior made in the action stage tend to be most visible and receive the greatest external recognition. People, including professionals, often erroneously equate action with change. As a consequence, they overlook the requisite work that prepares changers for action and the important efforts necessary to maintain the changes following action. (p. 1104)
Individuals who seek out professional help sometimes have already initiated behavioral changes in their lives; obtaining substance abuse treatment may be just one part of their change efforts. Studies have found that it is not unusual for clients to initiate abstinence days or even weeks before entering treatment (Maisto, Sobell, Sobell, Lei, & Sypora, 1988; Tucker, Vuchinich, & Pukish, 1995). According to DiClemente (1991), these are the clients who make therapists feel good about themselves; these are the “easy clients,” and the “miracle cures” (p. 199).
Clients already in action sometimes enter counseling to
(1) make a public commitment to action,
(2) obtain external confirmation of the plan,
(3) seek support and confidence, and
(4) create external monitors of their activity (DiClemente, 1991).
DiClemente (1991) maintained that the primary tasks of treatment personnel for helping clients in action is to identify ways to enhance their self-efficacy (e.g., introducing them to peer support networks) and, if possible, to remove any bureaucratic barriers that may impede their progress. Individuals are classified as in “action” if they successfully alter their behavior for a period of 1 day to 6 months. After 6 months of success, they are considered to have moved to the next stage (Prochaska & DiClemente, 1992).
Maintenance
In maintenance, people continue their efforts to prevent relapse and to consolidate gains made in treatment. Prochaska and DiClemente (1992) do not view maintenance as a static state but, rather, as a continuation of change. The threat of relapse becomes less and less intense with the passage of time. However, relapse to another stage remains a possibility.
Here, an important task for practitioners is to develop, with the client, a relapse prevention plan that anticipates, and protects against, “abstinence violation effects.” As discussed in Chapter 7, these are the intense, negative, emotional reactions, often involving self-downing, that many patients experience when they have a small setback or “lapse.” The significance of a lapse is exaggerated and leads to feelings of doom. In turn, these emotional reactions undermine self-efficacy and typically result in a more severe relapse than otherwise would be the case. One particularly deleterious consequence of abstinence violation effects is that out of embarrassment or shame, clients may conceal their return to drinking and/or drug use, or even worse, drop out of treatment. Relapse prevention plans must be realistic in educating clients about setbacks or “backsliding” and prescribe health-enhancing response options.
|
|
FIGURE 10.1. Prochaska and DiClemente’s six stages of change.
Figure 10.1 is the “wheel of change,” which shows how people cycle through the stages. Notice that precontemplation is not part of the motion of the wheel, which represents a static state. Most people who attempt change will move around the wheel several times before achieving permanent change (Miller & Rollnick, 2002).
OTHER depictions of the stages include:
|
|
|
|
|
|
|
|
|
|
|
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2015