|
|
|
GENDER DYSPHORIA is a psychological condition described in detail in the DSM-V. Almost all persons who describe themselves as “transgender” can be diagnosed as suffering from gender dysphoria employing the characteristics described in the DSM 5. The majority of children suffering from gender dysphoria will outgrow the symptoms without any treatment, and in time come to accept accept their natal gender, usually by adolescence.
DESPITE clear scientific evidence to the contrary (Sexuality and Gender 2016r; ACP 2017) and under increasing social pressure to normalize “Gender Theory” and transsexualism (Kheriaty), professional medical organizations have, with a few exceptions (ACP 2017), begun to regard hormonal and surgical “transition” for both adults and children as legitimate treatment for gender dysphoria (AAP, 2018; AJP, 2019; C.of E., 2017), often employing the rationale of suicide-prevention.
GENDER IDEOLOGY is a term used by Pope Francis in Amoris Laetitia (March 19, 2016) and elsewhere to describe the promotion and imposition on economically underdeveloped nations of non-traditional understandings of gender and sexual attraction, promoted chiefly by developed nations in Europe and by the United States and sometimes made a condition of economic aid. In 2017 the Vatican Congregation for Education expanded on Pope Francis’ observations in Amoris Laetitia and offered suggestions for dialogue and accompaniment in the are of education: Male and Female He Created Them.
The term “gender ideology” had been used of traditional sex-roles in a disparaging way in Sept 9. 2015 in in the Journal Sex Roles an article entitled, “Parents' Gender Ideology and Gendered Behavior as Predictors of Children's Gender-Role Attitudes: A Longitudinal Exploration” [https://pmc.ncbi.nlm.nih.gov/articles/PMC4945126/ ][https://link.springer.com/article/10.1007/s11199-015-0539-0 ].
Two feminist authors, Sonia Corrêa (2017) and Mariana Prandini Assis (2018) attribute to “vatican sources” the current negative use of he term by those who oppose the notion of self-determined gender-identity.
Sonia Corrêa, Nov. 12, 2017:https://blogs.lse.ac.uk/gender/2017/12/11/gender-ideology-tracking-its-origins-and-meanings-in-current-gender-politics/
Mariana Prandini Assis | Dec. 12, 2018 https://blog.feministische-studien.de/2018/12/gender-ideology-and-the-brazilian-elections/
Studies looking into the origins of the term “gender ideology” show that it did not emerge from civil society, but from the Vatican as early as the 1990s. As efforts to make gender equality a central focus of UN documents and policies progressed, a strategy that came to be known as gender mainstreaming, so did the attacks articulated by the Vatican — during the 1994 Cairo International Conference on Population and Development, and the Preparatory and Committee Meetings for the IV World Conference on Women (Beijing 1995). These confrontations gained a wider audience through publications by Catholic conservative groups based in the United States, such as “The Gender Agenda” by female Catholic pro-life journalist Dale O’Leary, and other Vatican documents that included references by Cardinal Joseph Ratzinger prior to his papacy. For the Vatican, the term gender would serve to deconstruct sex differences and lead to the dismantling of traditional family values, fostering “a war between the sexes, the devaluation of motherhood, the promotion of contraception and abortion, the acceptance of homosexual partnerships and parentage, and the decline of marriage,” as Professor of Law Mary Anne Case has shown in her study of the Vatican and gender.
 |
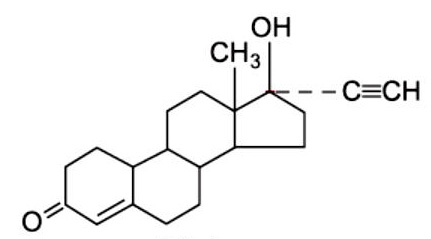 |
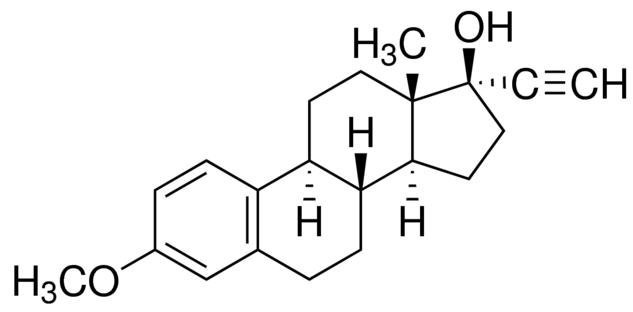
| MESTRANOL - A Progesterone | NORETHINDRONE - An Estrogen |
|
|
|
TESTOSTERONE - An Androgen |
RESOURCES and LINKS
“Treatment for Pediatric Gender Dysphoria, Review of Evidence and Best Practices,” Department of Health and Human Services, May 1, 2025, https://opa.hhs.gov/sites/default/files/2025-05/gender-dysphoria-report.pdf [local pdf]
United States Conference of Catholic Bishops. (2019). “Gender theory”/“Gender ideology” - Select Teaching Resources. https://www.usccb.org/resources/Gender-Ideology-Select-Teaching-Resources_0.pdf [local pdf]
United States Conference of Catholic Bishops. (March, 2023). “Doctrinal Note on The Moral Limits to Technological Manipulation of The Human Body” https://www.usccb.org/resources/Doctrinal%20Note%202023-03-20.pdf [local pdf]
“Sexuality and Gender”, The New Atlantis, Fall, 2016, Mayer, McHugh, “Sexuality and Gender, Findings from the Biological, Psychological, and Social Sciences”, https://www.thenewatlantis.com/publications/executive-summary-sexuality-and-gender [in PDF: Sexuality and Gender pdf]
McHugh, P. (2004). Surgical Sex: Why we stopped doing sex change operations. First Things. https://www.firstthings.com/article/2004/11/surgical-sex [local .doc]
National Catholic Bioethics Center. (n.d.). Resources on Bioethics Topics: Gender Identity & Being Transgender. https://www.ncbcenter.org/bioethics-resources
Cretella, M., et al. (2018). Gender Dysphoria in Children. American College of Pediatricians. https://acpeds.org/position-statements/gender-dysphoria-in-children
On Detransitioning: https://www.transgendertrend.com/detransition/
A community of people who question the medicalization of gender-atypical youth https://4thwavenow.com/
Courage and EnCourage: https://couragerc.org/ . EnCourage in the Diocese of Arlington -encourage@arlingtondiocese.org
Partners for Ethical Care: https://www.partnersforethicalcare.com/
Person and Identity: https://personandidentity.com/
Sex Change Regret: https://sexchangeregret.com/
Society for Evidence-Based Gender Medicine: https://segm.org/
Truth and Love: https://truthandlove.com/
Gender - A Wider Lens Podcast: https://gender-a-wider-lens.captivate.fm/
|
|
Emmaus, Ducio |
UNDERLYING these 8 steps is a twofold pastoral goal:
1. That the person be helped to SLOW DOWN, take things gradually, and not be pressured into making sudden, uninformed decisions that have negative long-term consequences
2. That the person eventually accept and discover the goodness and joy of their embodied gender.
1. JESUS CHRIST: Begin with PRAYER. Your professional competence is as a priest; not as a psychologist, social worker, or school counselor. Your competence is in the realms of evangelization, celebration of the sacraments, prayer, and balanced use of the means of grace.
2. LISTEN: Discover why the person desires “gender-affirming” treatment?. This will take time and more than one meeting.
3. ACCOMPANY: Be clear within yourself that you desire the good of the person. Collaborate, when appropriate with other professionals and competent persons, but do not simply refer and disappear from that person's life. Be VERY clear on how to contact you and how available you will be.
4. IMMEDIATE GOAL: Be clear within yourself - and do not hide from the person that your goal for them is that the person become comfortable in and accept their own body. Be honest about this and the Church's teaching, but not strident or condescending
5. ACKNOWLEDGE the TRUTH (and at lest the perceived “justice”) of the person's experience:
Do not tell lies or exaggerate . Acknowledge existence of studies supporting “gender-affirming treatment,” and GENTLY point out limitations (esp. long-term consequences).
Admit the pain of stereotypes, injustice, rejection, bullying, abandonment.
Acknowledge the physical and emotional stress of puberty and adolescence (especially the physical changes experienced by women)
Reinforce the truth that you desire the person's good and not merely compliance with moral norms.
6. DISCERN together with them how the person can best draw nearer Christ and avail themselves of the means of grace (prayer, sacramental life, private devotion)
7. ACTIVATE EXISTING COMMUNITY (parish, deanery, diocese): Encourage, form, seek out individuals and groups that encourage alternatives to transition: these include:
Family,
Parenthood,
Friendships.
ACTIVITIES the individual enjoys that AFFIRM their body and gender.
Recommend alternative points of view on Internet as person expresses interest. [Question: What is the feminine analog of sports as an alternative to gangs?]
8. FORM NEW EVANGELISTS. Be aware of and encourage individuals who can mentor or provide emotional support and living examples of alternatives to transition.
SCIENCE on
“TRANSGENDER”
CHILDREN
2017, Feb. 1
https://www.mercatornet.com/conjugality/view/how-the-transgender-agenda-harms-children/19384
On March 28, the US Supreme Court is due to hear a case about transgender bathroom access lodged by a Virginia student, Gavin Grimm. Born a girl, she decided in Year 9 that she was actually a boy. The local school board refused to let her use the boys’ toilets. She sued, and now the case has moved up to the Supreme Court (Gloucester County School Board v GG).
Amongst the briefs filed by “friends of the court” are a number of documents which contend that the transgender agenda will harm students.
Today we are publishing excerpts from a brief by Dr Judith Reisman, founder of the Child Protection Institute and a research professor at Liberty University School of Law. She is an internationally recognised expert on child sexual abuse and the influence of sexologist Alfred Kinsey.
* * * * * * *
As the [the Department of Justice and Department of Education Office of Civil Rights] instruct school districts, the purpose of Title IX is to provide a safe and nondiscriminatory environment for all students. Assuming that is true, then its interpretation of Title IX to include “gender identity,” and particularly to compel districts to permit access to sex-separate facilities based solely on perceived gender is in conflict with that purpose. Moreover, the Departments’ advocacy for recognition of “transgender” children fosters experimental, life-changing medical protocols that do not comply with the dictates of medical ethics. Most importantly, the Departments are sanctioning an agenda- driven ideology that threatens the physical, mental and emotional well-being of children.
Despite studies showing that 80 to 95 percent of children who report dissonance between their perceived gender and biological sex find that their perceived gender and biological sex correspond by late adolescence, medical protocols for “transgender” children are calling for earlier intervention with puberty- suppressing drugs and cross-sex hormones. These protocols create irreversible sterility and other life-changing effects to which the children, as minors with immature brains, are unable to give informed consent. Nor can their parents give “informed” consent to such protocols as the long-term consequences of these early interventions are unknown.
There is not a single large, randomized, controlled study that documents the alleged benefits and potential harms to gender-dysphoric children from pubertal suppression and decades of cross- sex hormone use. Nor is there a single long-term, large, randomized, controlled study that compares the outcomes of various toxic synthetic steroids.*
Nevertheless, gender clinics encourage treatments that will suppress puberty “to allow the gender dysphoric child time to explore gender identity free from the emotional distress triggered by the onset of secondary sex characteristics.” These treatments will condemn unknown numbers of children to sterility. In addition, use of puberty- suppressing drugs means that the children will never develop sperm or eggs.
Consequently, they would not even have the chance to harvest and preserve eggs or sperm for future use in assisted reproduction, an option some are given who go through puberty and then begin cross- sex hormones.
Furthermore, neuroscience has documented that children’s brains are cognitively immature until the early to mid- twenties. Scientists can digitally map how the brain develops, and have found that the portions of the brain that permit processing of complex concepts, such as “gender identity,” evaluating risk and making informed decisions are the last to mature, usually not until the early twenties. This means that children are not only legally, but cognitively incapable of giving informed consent to these treatments. Informed consent is a fundamental ethical requirement, particularly when, as is true for these early interventions, the treatment is irreversible and life-changing. The Nuremberg Code, developed in response to the human experimentation atrocities in Nazi Germany and still relied on in human research, states:
The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over- reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved, as to enable him to make an understanding and enlightened decision. This latter element requires that, before the acceptance of an affirmative decision by the experimental subject, there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person, which may possibly come from his participation in the experiment.
Children are not legally capable of giving consent. Even if it could be assumed, arguendo, that parents can consent on behalf of their children, they still cannot give informed consent because the hazards and the effects upon children’s health have not been scientifically determined and therefore cannot be known prior to treatment. By advocating for the inclusion of gender identity in Title IX for elementary and secondary students, the Departments are placing the government’s imprimatur on human experimentation and involuntary sterilization of children wholly bereft of informed consent. Such disregard for the health and safety of children as well as the rule of law should not be given any effect by this Court.
Notes
* Michelle Cretella, Gender Dysphoria in Children, American College of Pediatricians, (August 2016 - updated June 2017)
For the complete footnotes and bibliography in Dr Reisman's statement, see her amicus curiae brief.
Dr Judith Reisman served as Principal Investigator for the United States Department of Justice Office of Juvenile Justice on child sexual abuse and child pornography, and has provided expert reports and testimony in cases worldwide. She is an internationally recognized expert on the history, fraudulent research and societal effects of Dr Alfred Kinsey. She has authored five books and hundreds of articles dealing with the implications of Kinsey’s research on law and public policy.
- See more at: https://www.mercatornet.com/conjugality/view/how-the-transgender-agenda-harms-children/19384#sthash.datqCzpg.dpuf
https://www.nytimes.com/2022/06/15/magazine/gender-therapy.html
[...]European countries that had some liberal practices concerning young people seeking medication imposed new limits recently.
In February, [2022] the national health board in Sweden limited access to puberty suppressants and hormones before the age of 18 to “exceptional cases” and in research settings. The shift followed a Swedish public-television documentary that claimed doctors tried to hide spinal damage in a young patient whose bone density wasn’t adequately monitored.
Finland has similarly restricted access. One month after Sweden’s decision, the National Academy of Medicine in France called for “great medical caution” regarding treatment for young people, citing health risks (including for bone density and fertility) and noting the unexplained rise in trans-identified teenagers.
[...]
England’s National Health Service, too, asked for an independent review of the country’s gender-identity services (following a whistle-blower’s report in 2018 that the nation’s only pediatric clinic was fast-tracking young people into medical treatment and a lawsuit by a former patient — who later detransitioned — over the care she received there). Hilary Cass, a prominent pediatrician, is leading that effort. In a preliminary report in February that doesn’t make a final recommendation, she said the “lack of available high-level evidence” about puberty suppressants and hormone therapy for young people was “too inconclusive to form the basis of a policy position” on whether to continue the treatments. She also described a “mismatch” between the ethical responsibilities of clinicians to meet certain standards before a treatment and the distress some young people feel about a detailed assessment because they want “rapid access to physical interventions.” Like the SOC8 adolescent chapter, Cass suggested that the Dutch approach to assessment is the one best supported by the research.
Report shows falling number of youth
who identify as transgender
October 16, 2025
|
|
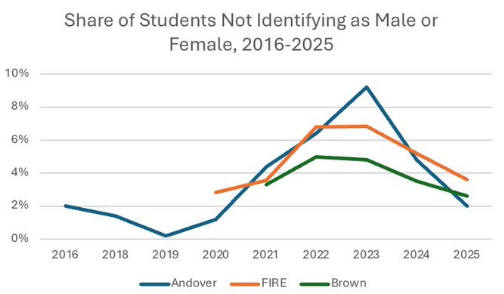
Eric Kaufmann, a professor of politics at the University of Buckingham (England), conducted his own analysis of a large survey of U.S. undergraduates — which included a question asking them to identify their gender. “This suggests that gender/sexual non-conformity will continue to fall,” Kaufmann wrote in an X post sharing the data.
The annual survey — College Free Speech Rankings — is conducted by the Foundation for Individual Rights and Expression (FIRE), headquartered in Philadelphia, Pennsylvania. The aim is to gather students’ opinions on freedom of speech, along with demographic information like gender. Kaufmann conducted his analyses using six years of demographic data from the survey, His independent report, “The Decline of Trans and Queer Identity among Young Americans,” was published by the Centre of Heterodox Social Science and has not been peer-reviewed.
In the 2025 survey of 68,000 students, only 3.6% of
respondents identified as a gender other than male or female.
The possible answers are[:]
• Man
• Woman
• Nonbinary
• Agender
• Genderqueer or genderfluid
• Unsure
• Prefer not to say
“Our survey looks at student attitudes for free expression and is conducted for that purpose,” FIRE told News Digital. “As a side effect of asking demographic questions of so many respondents, one can glean trends in demographics, as Professor Kaufmann has done here.”
https://zenit.org/2025/10/16/report-shows-falling-number-of-youth-who-identify-as-transgender/
According to new data from the American College Health Association, just 3.6% of college students now identify as a gender different from their biological sex ,
Over the past few years, the number of young Americans identifying as transgender or nonbinary has plummeted — a collapse that challenges the absurd cultural narrative that gender ideology represents a stable or permanent social shift. According to new data from the American College Health Association, just 3.6% of college students now identify as a gender different from their biological sex. That’s a sharp drop from 5.2% in 2024, and an even steeper fall from the 6.8% recorded in both 2022 and 2023.
The downward trend is consistent across nearly every demographic. Incoming freshmen — the group most likely to reflect new cultural trends — are now less likely than older students to identify as transgender or queer. In other words, the youngest generation on campus appears to be rejecting the gender confusion that was so heavily promoted in recent years. Meanwhile, the percentage of students identifying as heterosexual has begun to rise again, signaling a quiet return to normalcy after years of ideological pressure.
Importantly, the data show that this reversal isn’t being driven by religion or politics. The report found that rates of religiosity and political conservatism among students have remained largely stable. Instead, the shift appears tied to improvements in mental health. Anxiety and depression rates — both of which spiked during the pandemic — have begun to decline, and with that decline has come a steep reduction in the number of young people rejecting their biological sex. As psychological stability improves, gender experimentation is losing its grip.
For years, cultural elites, school systems, and social media platforms pushed the narrative that identifying as “trans” was brave, authentic, and liberating. But the truth is emerging: many young people were simply caught up in a socially contagious ideology. The more society normalizes mental health recovery and real self-acceptance, the less appealing the radical idea of “changing gender” becomes. This data doesn’t reflect a “loss of rights” — it reflects a generation waking up. The transgender movement sold itself as a permanent revolution, but the numbers tell another story. As the fad fades, what remains are the tragic consequences of irreversible medical interventions, social division, and institutional betrayal. The collapse in trans identification should serve as both a warning and a call to action: it’s time to protect children from ideological experimentation and restore truth, stability, and biological reality to public life.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 1990