|
|
|
|
|
|
CA
HEALTH and SAFETY Code
Relative
to PHYSICIAN-ASSISTED
SUICIDE
§443-443.22
442-442.7:
http://www.leginfo.ca.gov/cgi-bin/displaycode?section=hsc&group=00001-01000&file=442-442.7
443-443.22
http://www.leginfo.ca.gov/pub/15-16/bill/asm/ab_0001-0050/abx2_15_bill_20151005_chaptered.htm
http://www.leginfo.ca.gov/pub/15-16/bill/asm/ab_0001-0050/abx2_15_bill_20151005_chaptered.htm
CHAPTER 1
An act to add and repeal Part 1.85 (commencing with Section 443)
of Division 1 of the Health and Safety Code, relating to end of life.
[Approved by Governor October 05, 2015. Filed with Secretary of State October 05, 2015. ]
LEGISLATIVE COUNSEL'S
DIGEST
AB 15, Eggman. End of life.
Existing law authorizes an adult to give an individual health care instruction and to appoint an attorney to make health care decisions for that individual in the event of his or her incapacity pursuant to a power of attorney for health care.
This bill, until January 1, 2026, would enact the End of Life Option Act authorizing an adult who meets certain qualifications, and who has been determined by his or her attending physician to be suffering from a terminal disease, as defined, to make a request for a drug prescribed pursuant to these provisions for the purpose of ending his or her life. The bill would establish the procedures for making these requests. The bill would also establish specified forms to request an aid-in-dying drug, under specified circumstances, an interpreter declaration to be signed subject to penalty of perjury, thereby creating a crime and imposing a state-mandated local program, and a final attestation for an aid-in-dying drug. This bill would require specified information to be documented in the individual’s medical record, including, among other things, all oral and written requests for an aid-in-dying drug.
This bill would prohibit a provision in a contract, will, or other agreement from being conditioned upon, or affected by, a person making or rescinding a request for the above-described drug. The bill would prohibit the sale, procurement, or issuance of any life, health, or annuity policy, health care service plan contract, or health benefit plan, or the rate charged for any policy or plan contract, from being conditioned upon or affected by the request. The bill would prohibit an insurance carrier from providing any information in communications made to an individual about the availability of an aid-in-dying drug absent a request by the individual or his or her attending physician at the behest of the individual. The bill would also prohibit any communication from containing both the denial of treatment and information as to the availability of aid-in-dying drug coverage.
This bill would provide a person, except as provided, immunity from civil or criminal liability solely because the person was present when the qualified individual self-administered the drug, or the person assisted the qualified individual by preparing the aid-in-dying drug so long as the person did not assist with the ingestion of the drug, and would specify that the immunities and prohibitions on sanctions of a health care provider are solely reserved for conduct of a health care provider provided for by the bill. The bill would make participation in activities authorized pursuant to its provisions voluntary, and would make health care providers immune from liability for refusing to engage in activities authorized pursuant to its provisions. The bill would also authorize a health care provider to prohibit its employees, independent contractors, or other persons or entities, including other health care providers, from participating in activities under the act while on the premises owned or under the management or direct control of that prohibiting health care provider, or while acting within the course and scope of any employment by, or contract with, the prohibiting health care provider.
This bill would make it a felony to knowingly alter or forge a request for drugs to end an individual’s life without his or her authorization or to conceal or destroy a withdrawal or rescission of a request for a drug, if it is done with the intent or effect of causing the individual’s death. The bill would make it a felony to knowingly coerce or exert undue influence on an individual to request a drug for the purpose of ending his or her life, to destroy a withdrawal or rescission of a request, or to administer an aid-in-dying drug to an individual without their knowledge or consent. By creating a new crime, the bill would impose a state-mandated local program. The bill would provide that nothing in its provisions is to be construed to authorize ending a patient’s life by lethal injection, mercy killing, or active euthanasia, and would provide that action taken in accordance with the act shall not constitute, among other things, suicide or homicide.
This bill would require physicians to submit specified forms and information to the State Department of Public Health after writing a prescription for an aid-in-dying drug and after the death of an individual who requested an aid-in-dying drug. The bill would authorize the Medical Board of California to update those forms and would require the State Department of Public Health to publish the forms on its Internet Web site. The bill would require the department to annually review a sample of certain information and records, make a statistical report of the information collected, and post that report to its Internet Web site.
Existing constitutional provisions require that a statute that limits the right of access to the meetings of public bodies or the writings of public officials and agencies be adopted with findings demonstrating the interest protected by the limitation and the need for protecting that interest.
This bill would make legislative findings to that effect.
The California Constitution requires the state to reimburse local agencies and school districts for certain costs mandated by the state. Statutory provisions establish procedures for making that reimbursement.
This bill would provide that no reimbursement is required by this act for a specified reason.
Vote: majority Appropriation: no Fiscal Committee: yes Local Program: yes
SECTION 1.
Part 1.85 (commencing with Section 443) is added to Division 1 of the Health and Safety Code, to read:
PART 1.85. End of Life Option Act
443.
This part shall be known and may be cited as the End of Life Option Act.
443.1. [Definitions]
As used in this part, the following definitions shall apply:
(a) “Adult” means an individual 18 years of age or older.
(b) “Aid-in-dying drug” means a drug determined and prescribed by a physician for a qualified individual, which the qualified individual may choose to self-administer to bring about his or her death due to a terminal disease.
(c) “Attending physician” means the physician who has primary responsibility for the health care of an individual and treatment of the individual’s terminal disease.
(d) “Attending physician checklist and compliance form” means a form, as described in Section 443.22, identifying each and every requirement that must be fulfilled by an attending physician to be in good faith compliance with this part should the attending physician choose to participate.
(e) “Capacity to make medical decisions” means that, in the opinion of an individual’s attending physician, consulting physician, psychiatrist, or psychologist, pursuant to Section 4609 of the Probate Code, the individual has[:]
the ability to understand the nature and consequences of a health care decision,
the ability to understand its significant benefits, risks, and alternatives,
and the ability to make and communicate an informed decision to health care providers.
(f) “Consulting physician” means a physician who is independent from the attending physician and who is qualified by specialty or experience to make a professional diagnosis and prognosis regarding an individual’s terminal disease.
(g) “Department” means the State Department of Public Health.
(h) “Health care provider” or “provider of health care” means any person licensed or certified pursuant to Division 2 (commencing with Section 500) of the Business and Professions Code; any person licensed pursuant to the Osteopathic Initiative Act or the Chiropractic Initiative Act; any person certified pursuant to Division 2.5 (commencing with Section 1797) of this code; and any clinic, health dispensary, or health facility licensed pursuant to Division 2 (commencing with Section 1200) of this code.
(i) “Informed decision” means a decision by an individual with a terminal disease to request and obtain a prescription for a drug that the individual may self-administer to end the individual’s life, that is based on an understanding and acknowledgment of the relevant facts, and that is made after being fully informed by the attending physician of all of the following:
(1) The individual’s medical diagnosis and prognosis.
(2) The potential risks associated with taking the drug to be prescribed.
(3) The probable result of taking the drug to be prescribed.
(4) The possibility that the individual may choose not to obtain the drug or may obtain the drug but may decide not to ingest it.
(5) The feasible alternatives or additional treatment opportunities, including, but not limited to, comfort care, hospice care, palliative care, and pain control.
(j) “Medically confirmed” means the medical diagnosis and prognosis of the attending physician has been confirmed by a consulting physician who has examined the individual and the individual’s relevant medical records.
(k) “Mental health specialist assessment” means one or more consultations between an individual and a mental health specialist for the purpose of determining that the individual has the capacity to make medical decisions and is not suffering from impaired judgment due to a mental disorder.
(l) “Mental health specialist” means a psychiatrist or a licensed psychologist.
(m) “Physician” means a doctor of medicine or osteopathy currently licensed to practice medicine in this state.
(n) “Public place” means any street, alley, park, public building, any place of business or assembly open to or frequented by the public, and any other place that is open to the public view, or to which the public has access. [→ 443.5.a.5.A. on not ingesting there]
(o) “Qualified individual” means an adult who has the capacity to make medical decisions, is a resident of California, and has satisfied the requirements of this part in order to obtain a prescription for a drug to end his or her life.
(p) “Self-administer” means a qualified individual’s affirmative, conscious, and physical act of administering and ingesting the aid-in-dying drug to bring about his or her own death.
(q) “Terminal disease” means an incurable and irreversible disease that has been medically confirmed and will, within reasonable medical judgment, result in death within six months.
443.2. [Eligibility]
(a) An individual who is an adult with the capacity to make medical decisions and with a terminal disease may make a request to receive a prescription for an aid-in-dying drug if all of the following conditions are satisfied:
(1) The individual’s attending physician has diagnosed the individual with a terminal disease.
(2) The individual has voluntarily expressed the wish to receive a prescription for an aid-in-dying drug.
(3) The individual is a resident of California and is able to establish residency through any of the following means:
(A) Possession of a California driver license or other identification issued by the State of California.
(B) Registration to vote in California.
(C) Evidence that the person owns or leases property in California.
(D) Filing of a California tax return for the most recent tax year.
(4) The individual documents his or her request pursuant to the requirements set forth in Section 443.3.
(5) The individual has the physical and mental ability to self-administer the aid-in-dying drug.
(b) A person shall not be considered a “qualified individual” under the provisions of this part solely because of age or disability.
(c) A request for a prescription for an aid-in-dying drug under this part shall be made solely and directly by the individual diagnosed with the terminal disease and shall not be made on behalf of the patient, including, but not limited to, through a power of attorney, an advance health care directive, a conservator, health care agent, surrogate, or any other legally recognized health care decisionmaker.
443.3. [Written Request and Witness Requirements]
(a) An individual seeking to obtain a prescription for an aid-in-dying drug pursuant to this part shall submit two oral requests, a minimum of 15 days apart, and a written request to his or her attending physician. The attending physician shall directly, and not through a designee, receive all three requests required pursuant to this section.
(b) A valid written request for an aid-in-dying drug under subdivision (a) shall meet all of the following conditions:
(1) The request shall be in the form described in Section 443.11.
(2) The request shall be signed and dated, in the presence of two witnesses, by the individual seeking the aid-in-dying drug.
(3) The request shall be witnessed by at least two other adult persons who, in the presence of the individual, shall attest that to the best of their knowledge and belief the individual is all of the following:
(A) An individual who is personally known to them or has provided proof of identity.
(B) An individual who voluntarily signed this request in their presence.
(C) An individual whom they believe to be of sound mind and not under duress, fraud, or undue influence.
(D) Not an individual for whom either of them is the attending physician, consulting physician, or mental health specialist.
(c) Only one of the two witnesses at the time the written request is signed may:
(1) Be related to the qualified individual by blood, marriage, registered domestic partnership, or adoption or be entitled to a portion of the individual’s estate upon death.
(2) Own, operate, or be employed at a health care facility where the individual is receiving medical treatment or resides.
(d) The attending physician, consulting physician, or mental health specialist of the individual shall not be one of the witnesses required pursuant to paragraph (3) of subdivision (b).
443.4. [Right to Rescind Request]
(a) An individual may at any time withdraw or rescind his or her request for an aid-in-dying drug, or decide not to ingest an aid-in-dying drug, without regard to the individual’s mental state.
(b) A prescription for an aid-in-dying drug provided under this part may not be written without the attending physician directly, and not through a designee, offering the individual an opportunity to withdraw or rescind the request.
443.5.
(a) Before prescribing an aid-in-dying drug, the attending physician shall do all of the following:
(1) Make the initial determination of all of the following:
(A) (i) Whether the requesting adult has the capacity to make medical decisions.
(ii) If there are indications of a mental disorder, the physician shall refer the individual for a mental health specialist assessment.
(iii) If a mental health specialist assessment referral is made, no aid-in-dying drugs shall be prescribed until the mental health specialist determines that the individual has the capacity to make medical decisions and is not suffering from impaired judgment due to a mental disorder.
(B) Whether the requesting adult has a terminal disease.
(C) Whether the requesting adult has voluntarily made the request for an aid-in-dying drug pursuant to Sections 443.2 and 443.3.
(D) Whether the requesting adult is a qualified individual pursuant to subdivision (o) of Section 443.1.
(2) Confirm that the individual is making an informed decision by discussing with him or her all of the following:
(A) His or her medical diagnosis and prognosis.
(B) The potential risks associated with ingesting the requested aid-in-dying drug.
(C) The probable result of ingesting the aid-in-dying drug.
(D) The possibility that he or she may choose to obtain the aid-in-dying drug but not take it.
(E) The feasible alternatives or additional treatment options, including, but not limited to, comfort care, hospice care, palliative care, and pain control.
(3) Refer the individual to a consulting physician for medical confirmation of the diagnosis and prognosis, and for a determination that the individual has the capacity to make medical decisions and has complied with the provisions of this part.
(4) Confirm that the qualified individual’s request does not arise from coercion or undue influence by another person by discussing with the qualified individual, outside of the presence of any other persons, except for an interpreter as required pursuant to this part, whether or not the qualified individual is feeling coerced or unduly influenced by another person.
(5) Counsel the qualified individual about the importance of all of the following:
(A) Having another person present when he or she ingests the aid-in-dying drug prescribed pursuant to this part..
(B) Not ingesting the aid-in-dying drug in a public place
(C) Notifying the next of kin of his or her request for an aid-in-dying drug. A qualified individual who declines or is unable to notify next of kin shall not have his or her request denied for that reason.
(D) Participating in a hospice program.
(E) Maintaining the aid-in-dying drug in a safe and secure location until the time that the qualified individual will ingest it.
(6) Inform the individual that he or she may withdraw or rescind the request for an aid-in-dying drug at any time and in any manner.
(7) Offer the individual an opportunity to withdraw or rescind the request for an aid-in-dying drug before prescribing the aid-in-dying drug.
(8) Verify, immediately before writing the prescription for an aid-in-dying drug, that the qualified individual is making an informed decision.
(9) Confirm that all requirements are met and all appropriate steps are carried out in accordance with this part before writing a prescription for an aid-in-dying drug.
(10) Fulfill the record documentation required under Sections 443.8 and 443.19.
(11) Complete the attending physician checklist and compliance form, as described in Section 443.22, include it and the consulting physician compliance form in the individual’s medical record, and submit both forms to the State Department of Public Health.
(12) Give the qualified individual the final attestation form, with the instruction that the form be filled out and executed by the qualified individual within 48 hours prior to the qualified individual choosing to self-administer the aid-in-dying drug.
(b) If the conditions set forth in subdivision (a) are satisfied, the attending physician may deliver the aid-in-dying drug in any of the following ways:
(1) Dispensing the aid-in-dying drug directly, including ancillary medication intended to minimize the qualified individual’s discomfort, if the attending physician meets all of the following criteria:
(A) Is authorized to dispense medicine under California law.
(B) Has a current United States Drug Enforcement Administration (USDEA) certificate
(C) Complies with any applicable administrative rule or regulation.
(2) With the qualified individual’s written consent, contacting a pharmacist, informing the pharmacist of the prescriptions, and delivering the written prescriptions personally, by mail, or electronically to the pharmacist, who may dispense the drug to the qualified individual, the attending physician, or a person expressly designated by the qualified individual and with the designation delivered to the pharmacist in writing or verbally.
(c) Delivery of the dispensed drug to the qualified individual, the attending physician, or a person expressly designated by the qualified individual may be made by personal delivery, or, with a signature required on delivery, by United Parcel Service, United States Postal Service, Federal Express, or by messenger service.
443.6.
Before a qualified individual obtains an aid-in-dying drug from the attending physician, the consulting physician shall perform all of the following:
(a) Examine the individual and his or her relevant medical records.
(b) Confirm in writing the attending physician’s diagnosis and prognosis.
(c) Determine that the individual has the capacity to make medical decisions, is acting voluntarily, and has made an informed decision.
(d) If there are indications of a mental disorder, refer the individual for a mental health specialist assessment.
(e) Fulfill the record documentation required under this part.
(f) Submit the compliance form to the attending physician.
443.7.
Upon referral from the attending or consulting physician pursuant to this part, the mental health specialist shall:
(a) Examine the qualified individual and his or her relevant medical records.
(b) Determine that the individual has the mental capacity to make medical decisions, act voluntarily, and make an informed decision.
(c) Determine that the individual is not suffering from impaired judgment due to a mental disorder.
(d) Fulfill the record documentation requirements of this part.
443.8. [Documentation in Medical Record]
All of the following shall be documented in the individual’s medical record:
(a) All oral requests for aid-in-dying drugs.
(b) All written requests for aid-in-dying drugs.
(c) The attending physician’s diagnosis and prognosis, and the determination that a qualified individual has the capacity to make medical decisions, is acting voluntarily, and has made an informed decision, or that the attending physician has determined that the individual is not a qualified individual.
(d) The consulting physician’s diagnosis and prognosis, and verification that the qualified individual has the capacity to make medical decisions, is acting voluntarily, and has made an informed decision, or that the consulting physician has determined that the individual is not a qualified individual.
(e) A report of the outcome and determinations made during a mental health specialist’s assessment, if performed.
(f) The attending physician’s offer to the qualified individual to withdraw or rescind his or her request at the time of the individual’s second oral request.
(g) A note by the attending physician indicating that all requirements under Sections 443.5 and 443.6 have been met and indicating the steps taken to carry out the request, including a notation of the aid-in-dying drug prescribed.
443.9.
(a) Within 30 calendar days of writing a prescription for an aid-in-dying drug, the attending physician shall submit to the State Department of Public Health a copy of the qualifying patient’s written request, the attending physician checklist and compliance form, and the consulting physician compliance form.
(b) Within 30 calendar days following the qualified individual’s death from ingesting the aid-in-dying drug, or any other cause, the attending physician shall submit the attending physician followup form to the State Department of Public Health.
443.10.
A qualified individual may not receive a prescription for an aid-in-dying drug pursuant to this part unless he or she has made an informed decision. Immediately before writing a prescription for an aid-in-dying drug under this part, the attending physician shall verify that the individual is making an informed decision.
443.11.
(a) A request for an aid-in-dying drug as authorized by this part shall be in the following form:
|
REQUEST FOR AN AID-IN-DYING DRUG TO END MY LIFE IN A HUMANE AND DIGNIFIED MANNER I, ......................................................, am an adult of sound mind and a resident of the State of California. |
|
I am suffering from ................, which my attending physician has determined is in its terminal phase and which has been medically confirmed. |
|
I have been fully informed of my diagnosis and prognosis, the nature of the aid-in-dying drug to be prescribed and potential associated risks, the expected result, and the feasible alternatives or additional treatment options, including comfort care, hospice care, palliative care, and pain control. |
|
I request that my attending physician prescribe an aid-in-dying drug that will end my life in a humane and dignified manner if I choose to take it, and I authorize my attending physician to contact any pharmacist about my request. |
|
INITIAL ONE: |
|
............ I have informed one or more members of my family of my decision and taken their opinions into consideration. |
|
............ I have decided not to inform my family of my decision. |
|
............ I have no family to inform of my decision. |
|
I understand that I have the right to withdraw or rescind this request at any time. |
|
I understand the full import of this request and I expect to die if I take the aid-in-dying drug to be prescribed. My attending physician has counseled me about the possibility that my death may not be immediately upon the consumption of the drug. |
|
I make this request voluntarily, without reservation, and without being coerced. |
|
Signed:.............................................. |
|
Dated:............................................... |
|
DECLARATION OF WITNESSES |
|
We declare that the person signing this request: |
|
(a) is personally known to us or has provided proof of identity; |
|
(b) voluntarily signed this request in our presence; |
|
(c) is an individual whom we believe to be of sound mind and not under duress, fraud, or undue influence; and |
|
(d) is not an individual for whom either of us is the attending physician, consulting physician, or mental health specialist. |
|
............................Witness 1/Date |
|
............................Witness 2/Date |
|
NOTE: Only one of the two witnesses may be a relative (by blood, marriage, registered domestic partnership, or adoption) of the person signing this request or be entitled to a portion of the person’s estate upon death. Only one of the two witnesses may own, operate, or be employed at a health care facility where the person is a patient or resident. |
(b) (1) The written language of the request shall be written in the same translated language as any conversations, consultations, or interpreted conversations or consultations between a patient and his or her attending or consulting physicians.
(2) Notwithstanding paragraph (1), the written request may be prepared in English even when the conversations or consultations or interpreted conversations or consultations were conducted in a language other than English if the English language form includes an attached interpreter’s declaration that is signed under penalty of perjury. The interpreter’s declaration shall state words to the effect that:
|
I, (INSERT NAME OF INTERPRETER), am fluent in English and (INSERT TARGET LANGUAGE). |
|
On (insert date) at approximately (insert time), I read the “Request for an Aid-In-Dying Drug to End My Life” to (insert name of individual/patient) in (insert target language). |
|
Mr./Ms. (insert name of patient/qualified individual) affirmed to me that he/she understood the content of this form and affirmed his/her desire to sign this form under his/her own power and volition and that the request to sign the form followed consultations with an attending and consulting physician. |
|
I declare that I am fluent in English and (insert target language) and further declare under penalty of perjury that the foregoing is true and correct. |
|
Executed at (insert city, county, and state) on this (insert day of month) of (insert month), (insert year). |
|
X______Interpreter signature |
|
X______Interpreter printed name |
|
X______Interpreter address |
(3) An interpreter whose services are provided pursuant to paragraph (2) shall not be related to the qualified individual by blood, marriage, registered domestic partnership, or adoption or be entitled to a portion of the person’s estate upon death. An interpreter whose services are provided pursuant to paragraph (2) shall meet the standards promulgated by the California Healthcare Interpreting Association or the National Council on Interpreting in Health Care or other standards deemed acceptable by the department for health care providers in California.
(c) The final attestation form given by the attending physician to the qualified individual at the time the attending physician writes the prescription shall appear in the following form:
|
FINAL ATTESTATION FOR AN AID-IN-DYING DRUG TO END MY LIFE IN A HUMANE AND DIGNIFIED MANNER I, ......................................................, am an adult of sound mind and a resident of the State of California. |
|
I am suffering from ................, which my attending physician has determined is in its terminal phase and which has been medically confirmed. |
|
I have been fully informed of my diagnosis and prognosis, the nature of the aid-in-dying drug to be prescribed and potential associated risks, the expected result, and the feasible alternatives or additional treatment options, including comfort care, hospice care, palliative care, and pain control. |
|
I have received the aid-in-dying drug and am fully aware that this aid-in-dying drug will end my life in a humane and dignified manner. |
|
INITIAL ONE: |
|
............ I have informed one or more members of my family of my decision and taken their opinions into consideration. |
|
............ I have decided not to inform my family of my decision. |
|
............ I have no family to inform of my decision. |
|
My attending physician has counseled me about the possibility that my death may not be immediately upon the consumption of the drug. |
|
I make this decision to ingest the aid-in-dying drug to end my life in a humane and dignified manner. I understand I still may choose not to ingest the drug and by signing this form I am under no obligation to ingest the drug. I understand I may rescind this request at any time. |
|
Signed:.............................................. |
|
Dated:............................................... |
|
Time:................................................. |
(1) Within 48 hours prior to the individual self-administering the aid-in-dying drug, the individual shall complete the final attestation form. If aid-in-dying medication is not returned or relinquished upon the patient’s death as required in Section 443.20, the completed form shall be delivered by the individual’s health care provider, family member, or other representative to the attending physician to be included in the patient’s medical record.
(2) Upon receiving the final attestation form the attending physician shall add this form to the medical records of the qualified individual.
443.12.
(a) A provision in a contract, will, or other agreement executed on or after January 1, 2016, whether written or oral, to the extent the provision would affect whether a person may make, withdraw, or rescind a request for an aid-in-dying drug is not valid.
(b) An obligation owing under any contract executed on or after January 1, 2016, may not be conditioned or affected by a qualified individual making, withdrawing, or rescinding a request for an aid-in-dying drug.
443.13.
(a) (1) The sale, procurement, or issuance of a life, health, or annuity policy, health care service plan contract, or health benefit plan, or the rate charged for a policy or plan contract may not be conditioned upon or affected by a person making or rescinding a request for an aid-in-dying drug.
(2) Pursuant to Section 443.18, death resulting from the self-administration of an aid-in-dying drug is not suicide, and therefore health and insurance coverage shall not be exempted on that basis.
(b) Notwithstanding any other law, a qualified individual’s act of self-administering an aid-in-dying drug shall not have an effect upon a life, health, or annuity policy other than that of a natural death from the underlying disease.
(c) An insurance carrier shall not provide any information in communications made to an individual about the availability of an aid-in-dying drug absent a request by the individual or his or her attending physician at the behest of the individual. Any communication shall not include both the denial of treatment and information as to the availability of aid-in-dying drug coverage. For the purposes of this subdivision, “insurance carrier” means a health care service plan as defined in Section 1345 of this code or a carrier of health insurance as defined in Section 106 of the Insurance Code.
443.14.
(a) Notwithstanding any other law, a person shall not be subject to civil or criminal liability solely because the person was present when the qualified individual self-administers the prescribed aid-in-dying drug. A person who is present may, without civil or criminal liability, assist the qualified individual by preparing the aid-in-dying drug so long as the person does not assist the qualified person in ingesting the aid-in-dying drug.
(b) A health care provider or professional organization or association shall not subject an individual to censure, discipline, suspension, loss of license, loss of privileges, loss of membership, or other penalty for participating in good faith compliance with this part or for refusing to participate in accordance with subdivision (e).
(c) Notwithstanding any other law, a health care provider shall not be subject to civil, criminal, administrative, disciplinary, employment, credentialing, professional discipline, contractual liability, or medical staff action, sanction, or penalty or other liability for participating in this part, including, but not limited to, determining the diagnosis or prognosis of an individual, determining the capacity of an individual for purposes of qualifying for the act, providing information to an individual regarding this part, and providing a referral to a physician who participates in this part. Nothing in this subdivision shall be construed to limit the application of, or provide immunity from, Section 443.16 or 443.17.
(d) (1) A request by a qualified individual to an attending physician to provide an aid-in-dying drug in good faith compliance with the provisions of this part shall not provide the sole basis for the appointment of a guardian or conservator.
(2) No actions taken in compliance with the provisions of this part shall constitute or provide the basis for any claim of neglect or elder abuse for any purpose of law.
(e) (1) Participation in activities authorized pursuant to this part shall be voluntary. Notwithstanding Sections 442 to 442.7, inclusive, a person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.
(2) Notwithstanding any other law, a health care provider is not subject to civil, criminal, administrative, disciplinary, employment, credentialing, professional discipline, contractual liability, or medical staff action, sanction, or penalty or other liability for refusing to participate in activities authorized under this part, including, but not limited to, refusing to inform a patient regarding his or her rights under this part, and not referring an individual to a physician who participates in activities authorized under this part.
(3) If a health care provider is unable or unwilling to carry out a qualified individual’s request under this part and the qualified individual transfers care to a new health care provider, the individual may request a copy of his or her medical records pursuant to law.
443.15.
(a) Subject to subdivision (b), notwithstanding any other law, a health care provider may prohibit its employees, independent contractors, or other persons or entities, including other health care providers, from participating in activities under this part while on premises owned or under the management or direct control of that prohibiting health care provider or while acting within the course and scope of any employment by, or contract with, the prohibiting health care provider.
(b) A health care provider that elects to prohibit its employees, independent contractors, or other persons or entities, including health care providers, from participating in activities under this part, as described in subdivision (a), shall first give notice of the policy prohibiting participation under this part to the individual or entity. A health care provider that fails to provide notice to an individual or entity in compliance with this subdivision shall not be entitled to enforce such a policy against that individual or entity.
(c) Subject to compliance with subdivision (b), the prohibiting health care provider may take action, including, but not limited to, the following, as applicable, against any individual or entity that violates this policy:
(1) Loss of privileges, loss of membership, or other action authorized by the bylaws or rules and regulations of the medical staff.
(2) Suspension, loss of employment, or other action authorized by the policies and practices of the prohibiting health care provider.
(3) Termination of any lease or other contract between the prohibiting health care provider and the individual or entity that violates the policy.
(4) Imposition of any other nonmonetary remedy provided for in any lease or contract between the prohibiting health care provider and the individual or entity in violation of the policy.
(d) Nothing in this section shall be construed to prevent, or to allow a prohibiting health care provider to prohibit, any other health care provider, employee, independent contractor, or other person or entity from any of the following:
(1) Participating, or entering into an agreement to participate, in activities under this part, while on premises that are not owned or under the management or direct control of the prohibiting provider or while acting outside the course and scope of the participant’s duties as an employee of, or an independent contractor for, the prohibiting health care provider.
(2) Participating, or entering into an agreement to participate, in activities under this part as an attending physician or consulting physician while on premises that are not owned or under the management or direct control of the prohibiting provider.
(e) In taking actions pursuant to subdivision (c), a health care provider shall comply with all procedures required by law, its own policies or procedures, and any contract with the individual or entity in violation of the policy, as applicable.
(f) For purposes of this section:
(1) “Notice” means a separate statement in writing advising of the prohibiting health care provider policy with respect to participating in activities under this part.
(2) “Participating, or entering into an agreement to participate, in activities under this part” means doing or entering into an agreement to do any one or more of the following:
(A) Performing the duties of an attending physician as specified in Section 443.5.
(B) Performing the duties of a consulting physician as specified in Section 443.6.
(C) Performing the duties of a mental health specialist, in the circumstance that a referral to one is made.
(D) Delivering the prescription for, dispensing, or delivering the dispensed aid-in-dying drug pursuant to paragraph (2) of subdivision (b) of, and subdivision (c) of, Section 443.5.
(E) Being present when the qualified individual takes the aid-in-dying drug prescribed pursuant to this part.
(3) “Participating, or entering into an agreement to participate, in activities under this part” does not include doing, or entering into an agreement to do, any of the following:
(A) Diagnosing whether a patient has a terminal disease, informing the patient of the medical prognosis, or determining whether a patient has the capacity to make decisions.
(B) Providing information to a patient about this part.
(C) Providing a patient, upon the patient’s request, with a referral to another health care provider for the purposes of participating in the activities authorized by this part.
(g) Any action taken by a prohibiting provider pursuant to this section shall not be reportable under Sections 800 to 809.9, inclusive, of the Business and Professions Code. The fact that a health care provider participates in activities under this part shall not be the sole basis for a complaint or report by another health care provider of unprofessional or dishonorable conduct under Sections 800 to 809.9, inclusive, of the Business and Professions Code.
(h) Nothing in this part shall prevent a health care provider from providing an individual with health care services that do not constitute participation in this part.
443.16.
(a) A health care provider may not be sanctioned for any of the following:
(1) Making an initial determination pursuant to the standard of care that an individual has a terminal disease and informing him or her of the medical prognosis.
(2) Providing information about the End of Life Option Act to a patient upon the request of the individual.
(3) Providing an individual, upon request, with a referral to another physician.
(b) A health care provider that prohibits activities under this part in accordance with Section 443.15 shall not sanction an individual health care provider for contracting with a qualified individual to engage in activities authorized by this part if the individual health care provider is acting outside of the course and scope of his or her capacity as an employee or independent contractor of the prohibiting health care provider.
(c) Notwithstanding any contrary provision in this section, the immunities and prohibitions on sanctions of a health care provider are solely reserved for actions of a health care provider taken pursuant to this part. Notwithstanding any contrary provision in this part, health care providers may be sanctioned by their licensing board or agency for conduct and actions constituting unprofessional conduct, including failure to comply in good faith with this part.
443.17.
(a) Knowingly altering or forging a request for an aid-in-dying drug to end an individual’s life without his or her authorization or concealing or destroying a withdrawal or rescission of a request for an aid-in-dying drug is punishable as a felony if the act is done with the intent or effect of causing the individual’s death.
(b) Knowingly coercing or exerting undue influence on an individual to request or ingest an aid-in-dying drug for the purpose of ending his or her life or to destroy a withdrawal or rescission of a request, or to administer an aid-in-dying drug to an individual without his or her knowledge or consent, is punishable as a felony.
(c) For purposes of this section, “knowingly” has the meaning provided in Section 7 of the Penal Code.
(d) The attending physician, consulting physician, or mental health specialist shall not be related to the individual by blood, marriage, registered domestic partnership, or adoption, or be entitled to a portion of the individual’s estate upon death.
(e) Nothing in this section shall be construed to limit civil liability.
(f) The penalties in this section do not preclude criminal penalties applicable under any law for conduct inconsistent with the provisions of this section.
443.18.
Nothing in this part may be construed to authorize a physician or any other person to end an individual’s life by lethal injection, mercy killing, or active euthanasia. Actions taken in accordance with this part shall not, for any purposes, constitute suicide, assisted suicide, homicide, or elder abuse under the law.
443.19. [Documentation and Statistics]
(a) The State Department of Public Health shall collect and review the information submitted pursuant to Section 443.9. The information collected shall be confidential and shall be collected in a manner that protects the privacy of the patient, the patient’s family, and any medical provider or pharmacist involved with the patient under the provisions of this part. The information shall not be disclosed, discoverable, or compelled to be produced in any civil, criminal, administrative, or other proceeding.
(b) On or before July 1, 2017, and each year thereafter, based on the information collected in the previous year, the department shall create a report with the information collected from the attending physician followup form and post that report to its Internet Web site. The report shall include, but not be limited to, all of the following based on the information that is provided to the department and on the department’s access to vital statistics:
(1) The number of people for whom an aid-in-dying prescription was written.
(2) The number of known individuals who died each year for whom aid-in-dying prescriptions were written, and the cause of death of those individuals.
(3) For the period commencing January 1, 2016, to and including the previous year, cumulatively, the total number of aid-in-dying prescriptions written, the number of people who died due to use of aid-in-dying drugs, and the number of those people who died who were enrolled in hospice or other palliative care programs at the time of death.
(4) The number of known deaths in California from using aid-in-dying drugs per 10,000 deaths in California.
(5) The number of physicians who wrote prescriptions for aid-in-dying drugs.
(6) Of people who died due to using an aid-in-dying drug, demographic percentages organized by the following characteristics:
(A) Age at death.
(B) Education level.
(C) Race.
(D) Sex.
(E) Type of insurance, including whether or not they had insurance.
(F) Underlying illness.
(c) The State Department of Public Health shall make available the attending physician checklist and compliance form, the consulting physician compliance form, and the attending physician followup form, as described in Section 443.22, by posting them on its Internet Web site.
443.20.
A person who has custody or control of any unused aid-in-dying drugs prescribed pursuant to this part after the death of the patient shall personally deliver the unused aid-in-dying drugs for disposal by delivering it to the nearest qualified facility that properly disposes of controlled substances, or if none is available, shall dispose of it by lawful means in accordance with guidelines promulgated by the California State Board of Pharmacy or a federal Drug Enforcement Administration approved take-back program.
443.21.
Any governmental entity that incurs costs resulting from a qualified individual terminating his or her life pursuant to the provisions of this part in a public place shall have a claim against the estate of the qualified individual to recover those costs and reasonable attorney fees related to enforcing the claim.
443.215.
This part shall remain in effect only until January 1, 2026, and as of that date is repealed, unless a later enacted statute, that is enacted before January 1, 2026, deletes or extends that date.
443.22.
(a) The Medical Board of California may update the attending physician checklist and compliance form, the consulting physician compliance form, and the attending physician followup form, based on those provided in subdivision (b). Upon completion, the State Department of Public Health shall publish the updated forms on its Internet Web site.
(b) Unless and until updated by the Medical Board of California pursuant to this section, the attending physician checklist and compliance form, the consulting physician compliance form, and the attending physician followup form shall be in the following form:
PRINTER PLEASE NOTE: TIP-IN MATERIAL TO BE INSERTED
The Legislature finds and declares that Section 1 of this act, which adds Section 443.19 to the Health and Safety Code, imposes a limitation on the public’s right of access to the meetings of public bodies or the writings of public officials and agencies within the meaning of Section 3 of Article I of the California Constitution. Pursuant to that constitutional provision, the Legislature makes the following findings to demonstrate the interest protected by this limitation and the need for protecting that interest:
(a) Any limitation to public access to personally identifiable patient data collected pursuant to Section 443.19 of the Health and Safety Code as proposed to be added by this act is necessary to protect the privacy rights of the patient and his or her family.
(b) The interests in protecting the privacy rights of the patient and his or her family in this situation strongly outweigh the public interest in having access to personally identifiable data relating to services.
(c) The statistical report to be made available to the public pursuant to subdivision (b) of Section 443.19 of the Health and Safety Code is sufficient to satisfy the public’s right to access.
The provisions of this part are severable. If any provision of this part or its application is held invalid, that invalidity shall not affect other provisions or applications that can be given effect without the invalid provision or application.
No reimbursement is required by this act pursuant to Section 6 of Article XIII B of the California Constitution because the only costs that may be incurred by a local agency or school district will be incurred because this act creates a new crime or infraction, eliminates a crime or infraction, or changes the penalty for a crime or infraction, within the meaning of Section 17556 of the Government Code, or changes the definition of a crime within the meaning of Section 6 of Article XIII B of the California Constitution.
Senator Susan Eggman (D) introduced an amendment to California’s law, End of Life, SB380. Effective beginning January 1, 2022, the amendment:
• Reduces the waiting period between the 1st and 2nd oral request from 15 days to 48 hours;
• Eliminates the final attestation form;
• Requires physicians who cannot or will not support patient requests to tell the patient they will not support them, document the patient’s request and provider’s notice of rejection in the patient’s medical record, and transfer the relevant medical record upon request;
• Prohibits a health care provider or health care entity from engaging in false, misleading, or deceptive practices relating to their willingness to qualify an individual or provide a prescription for an aid-in-dying medication to a qualified individual;
• Requires health care entities to post their current policy regarding medical aid in dying on their internet website;
• Extends the law’s repeal clause to January 1, 2031.
DRUGS,
DISCUSSION
and STATISTICS
Physician-assisted Suicide:
Ongoing Challenges for
Pharmacists
Jennifer Fass and Andrea Fass
American Journal of Health-System Pharmacy
http://www.medscape.com/viewarticle/742070_3
Am J Health Syst Pharm. 2011;68(9):846-849.
Drug Information Issues
Currently in Oregon, secobarbital is the medication most commonly prescribed for physician-assisted suicide, followed by pentobarbital.[3] The lethal dose prescribed is typically 9 g of secobarbital in capsules or 10 g of pentobarbital liquid, to be consumed at one time.[4–6] The contents of the secobarbital capsules or the pentobarbital liquid should be mixed with a sweet substance such as juice to mask the bitter taste. Until the time of use, the medication must be stored out of reach of children and kept away from others to prevent unintentional overdose or abuse.
The pharmacist or physician should instruct patients to take the lethal dose on an empty stomach to increase the rate of absorption.[7] The typical dose of pentobarbital as an oral hypnotic for adults is 100–200 mg at bedtime, and that of secobarbital is 100 mg orally at bedtime.
Patients receiving the lethal dose of secobarbital or pentobarbital should be instructed to take an antiemetic (e.g., metoclopramide) about one hour before ingesting the barbiturate to prevent nausea and vomiting.[6]
Cases of vomiting after taking an antiemetic have been reported; in the event of vomiting after medication ingestion, patients should be instructed to have a family member contact the attending physician to determine the course of action.[2]
Also, patients should be instructed that if they decide not to end their life after ingesting the medication, they must contact emergency medical services to begin lifesaving measures.[2]
Patients need to be informed of appropriate disposal methods in case the medication is not taken; the Food and Drug Administration provides guidance on that issue.[8] Secobarbital and pentobarbital are not among the medications recommended for disposal by flushing, and they should be placed in the household trash after mixing with an unpalatable substance such as coffee grounds. Unused medications also can be brought to a drug “take-back” program involving law enforcement personnel. Patients are not permitted to return controlled-substance medications to a pharmacy.[9]
Proper reporting by pharmacists to the Oregon Department of Human Services is mandated by the DWDA so the agency can collect information and publish an annual statistical report.[10] Pharmacists are required to complete and submit, within 10 calendar days of dispensing a lethal medication dose, a pharmacy dispensing record form with the following information: the patient’s name and date of birth; the prescribing physician’s name and phone number; the pharmacist’s name, address, and phone number; the medication and quantity dispensed; and the dates the prescription was written and dispensed.
Since the Oregon DWDA took effect in 1997, 460 patients have died by self-administration of a lethal dose of a prescription medication.[11]
In 2009, 95 prescriptions were written for lethal medications, resulting in 59 deaths (in the remaining cases, the medication was not ingested).
About 80% of the patients had malignant cancer, and the most commonly ingested lethal medication was secobarbital (85% of cases).
About 78% of the patients were 55–84 years of age. The time from ingestion to death ranged from two minutes to 4.5 days.[3,11]
The state of Washington passed a DWDA that mirrors Oregon’s statute and became effective in March 2009. Participating pharmacists in Washington must submit the pharmacy dispensing record within 30 days of dispensing to the registrar of the state’s Center for Health Statistics.[12] The Washington State Department of Health issued its first report in March 2010. According to the report, a lethal dose of medication, usually secobarbital (89% of cases), was dispensed to 63 patients by 29 different pharmacists.[13] Of those 63 patients, 36 individuals died as a result of ingesting the medication, 7 died without ingestion, and data are missing for 4 individuals; data collection for the remaining 16 individuals is pending. The most common reported illnesses were cancer (79%), respiratory disease or other illnesses (12%), and amyotrophic lateral sclerosis (9%). The required dispensing record form was submitted to the Department of Health for all 63 patients. The reported times from medication ingestion to death ranged from nine minutes to 28 hours.
Pharmacists and physicians cannot be held liable for participating in physician-assisted suicide in Oregon and Washington if they adhere to the legal requirements.[1,12] In December 2008, the Montana supreme court ruled that physician-assisted suicide is legal after a patient with terminal cancer sued the state in the case of Baxter v. Montana,[14,15] but legal requirements such as reporting regulations have not been established. A bill to ban the practice in Montana was introduced in the state legislative session on January 6, 2011, and a hearing scheduled for late January. Montana still has not established rules and regulations.
1. The Oregon Death with Dignity Act: Oregon revised statutes. www.oregon.gov/DHS/ph/pas/docs/statute.pdf (accessed 2010 Dec 27).
2. Task Force to Improve the Care of Terminally-Ill Oregonians. The Oregon Death with Dignity Act: a guidebook for health care professionals. www.ohsu.edu/xd/education/continuing-education/center-forethics/ethics-outreach/upload/Oregon-Death-with-Dignity-Act-Guidebook.pdf (accessed 2010 Dec 27).
3. Oregon Department of Human Services. 2009 summary of Oregon’s Death with Dignity Act. www.oregon.gov/DHS/ph/pas/docs/year12.pdf (accessed 2010 Dec 27).
4. Oregon Department of Human Services. Fifth annual report on Oregon’s Death with Dignity Act. www.oregon.gov/DHS/ph/pas/docs/year5.pdf (accessed 2010 Dec 27).
5. Okie S. Physician-assisted suicide— Oregon and beyond. N Engl J Med. 2005; 352:1627-30.
6. Wineberg H. Oregon’s Death with Dignity Act: fourteen months and counting. Arch Intern Med. 2000; 160:21–3.
7. McEvoy GK, Snow EK. Barbiturates. www.ahfsdruginformation.com/support/not_in_print/a382386.aspx (accessed 2011 Jan 14).
8. U.S. Food and Drug Administration. Disposal by flushing of certain unused medicines: what you should know. www. fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/EnsuringSafeUseofMedicine/
9. Drug Enforcement Administration. Office of Diversion Control questions & answers. www.deadiversion.usdoj.gov/faq/general.htm (accessed 2010 Dec 27).
10. Oregon Department of Human Services. Pharmacy dispensing record. http://egov.oregon.gov/DHS/ph/pas/docs/pharform.pdf (accessed 2010 Dec 27).
11. Oregon Department of Human Services. Table 1. Characteristics and end-of-life care of 460 DWDA patients who died after ingesting a lethal dose of medication, by year, Oregon, 1998–2009. www.oregon.gov/DHS/ph/pas/docs/yr12-tbl-1.pdf (accessed 2010 Dec 27).
12. The Washington Death with Dignity Act, chap. 70.245 RCW. http://apps.leg.wa.gov/RCW/default.aspx?cite=70.245 (accessed 2010 Dec 27).
13. Washington State Department of Health. Washington State Department of Health 2009 Death with Dignity Act report executive summary. www.doh.wa.gov/dwda/forms/DWDA_2009.pdf (accessed 2010 Dec 27).
14. Robert Baxter v. State of Montana andSteve Bullock. In the Supreme Court of the State of Montana (No. DA 09-0051), brief amicus curiae of International Task Force on Euthanasia & Assisted Suicide (LexisNexis Academic; accessed 2010 Jun 3).
15. The Associated Press. Montana judge endorses right to assisted suicide. www.nytimes.com/2008/12/07/health/07montana.html?_r=1&pagewanted=print (accessed 2010 Dec 27).
16. American Pharmacists Association. Code of ethics for pharmacists. www.pharmacist.com/AM/Template.cfm?Section=Code_of_Ethics_for_Pharmacists&TEMPLATE=/CM/HTMLDisplay.cfm&CONTENTID=2654 (accessed 2010 Dec 27).
17. American Pharmaceutical Association. Report of the 2004 APhA house of delegates. J Am Pharm Assoc. 2004; 44:551–6.
18. American Society of Health-System Pharmacists. ASHP statement on pharmacist decision making on assisted suicide. Am J Health-Syst Pharm. 1999; 56:1661–4.
19. Baluch WM. Perplexed about ASHP council’s perspective on assisted-suicide policy. Am J Health-Syst Pharm. 2000; 57:998–9. Comment.
20. Wernow JR, Grant DG. Dispensing with conscience: a legal and ethical assessment. Ann Pharmacother. 2008; 42:1669–78.
21. Oregon Department of Human Services. FAQs about the Death with Dignity Act. www.oregon.gov/DHS/ph/pas/faqs.shtml (accessed 2010 Dec 27).
22. Washington State Hospital Association. Death with Dignity Act. www.wsha.org/page.cfm?ID=0302 (accessed 2010 Dec 27).
23. Compassion & Choices. About Compassion & Choices. www.compassionandchoices.org/learn (accessed 2010 Dec 27).
24. Rupp MT. Physician-assisted suicide and the issues it raises for pharmacists. Am J Health-Syst Pharm. 1995; 52:1455–60.
25. Veatch RM. The pharmacist and assisted suicide. Am J Health-Syst Pharm. 1999; 56:260–6.
26. Rupp MT, Isenhower HL. Pharmacists’ attitudes toward physician-assisted suicide. Am J Hosp Pharm. 1994; 51:69–74.
27. Vivian JC, Slaughter RL, Calissi P. Michigan pharmacists’ attitudes about medically-assisted suicide. J Mich Pharm. 1993; 31:490–3.
28. Death with Dignity National Center. The dignity report: DDNC spring 2010 newsletter. www.deathwithdignity.org/2010/03/24/spring-2010-newsletter/ (accessed 2010 Dec 27).
29. Purdue Pharma. Medical education resource catalog. www.purduepharmamededresources.com (accessed 2010 Dec 27).
30. American Academy of Pain Management. American Academy of Pain Management Learning Center. https://aapm.cecity.com/ce-bin/owa/pkg_explorer_search.prof_sel ect?ip_company_code=AAPM&cookie=34933145&ip_subj ect=125451&v_url=pkg_curriculum%2emycurriculum_w%3fv_company_code%3dAAPM%26cookie%3d34933145 (accessed 2010 Dec 27).
31. Death with Dignity National Center. Death with dignity must be made available in all 50 states. www.deathwithdignity.org/2009/02/26/press-releasere-final-exit/ (accessed 2010 Dec 27).
PHYSICIAN-ASSISTED
SUICIDE
FAST
FACTS
[And Statistics]
CNN Library
Updated 3:25 PM ET, Tue October 6, 2015
Story highlights
· Legal in Montana, Oregon, Vermont, Washington and Bernalillo County in New Mexico.
· The process of reporting applications and deaths varies by state.
· The U.S. Supreme Court ruled that state laws banning physician-assisted suicide do not violate the Constitution.
(CNN)Physician-assisted suicide is legal in five U.S. states. It is an option given to individuals by state law in Oregon, Vermont, Washington and California. It is an option given to individuals in Montana via court decision. Individuals must have a terminal illness as well as a prognosis of six months or less to live. Physicians cannot be prosecuted for prescribing medications to hasten death.
Mandated by State Law:
Oregon
Vermont
Washington
California
Mandated by Court Ruling:
Montana
Other Facts:
The specific method in each state varies, but mainly involves a prescription
from a licensed physician approved by the state in which the patient is a
resident.
Physician-assisted suicide differs from euthanasia, which is defined as the act of assisting people with their death in order to end their suffering, but without the backing of a controlling legal authority.
In Oregon, “the physician must be a Doctor of Medicine (M.D.) or Doctor of Osteopathy (D.O.) licensed to practice medicine by the Board of Medical Examiners for the State of Oregon. The physician must also be willing to participate in the Act.”
In Vermont, ”only a doctor of medicine or osteopathy licensed to practice medicine in Washington may write this prescription...A physician, nurse, pharmacist, or other person shall not be under any duty, by law or contract, to participate in the provision of a lethal dose of medication to a patient.”
In Washington, “only a doctor of medicine or osteopathy licensed to practice medicine in Washington may write this prescription...participation is entirely voluntary. Health care providers are not required to provide prescriptions or medications to qualified patients.”
In California, “ An individual seeking to obtain a prescription for an aid-in-dying drug...shall submit two oral requests, a minimum of 15 days apart, and a written request to his or her attending physician. The attending physician shall directly, and not through a designee, receive all three requests required pursuant to this section.”
PDF with DETAILED INFORMATION on OREGON
CALIFORNIA: 2017 - 191Rx 111 Died; 2018 - 452 Rx. 337 Died;
Statistics:
The process of reporting applications and deaths varies by state. Only those
states where physician-assisted suicide is mandated by law have a reporting
process.
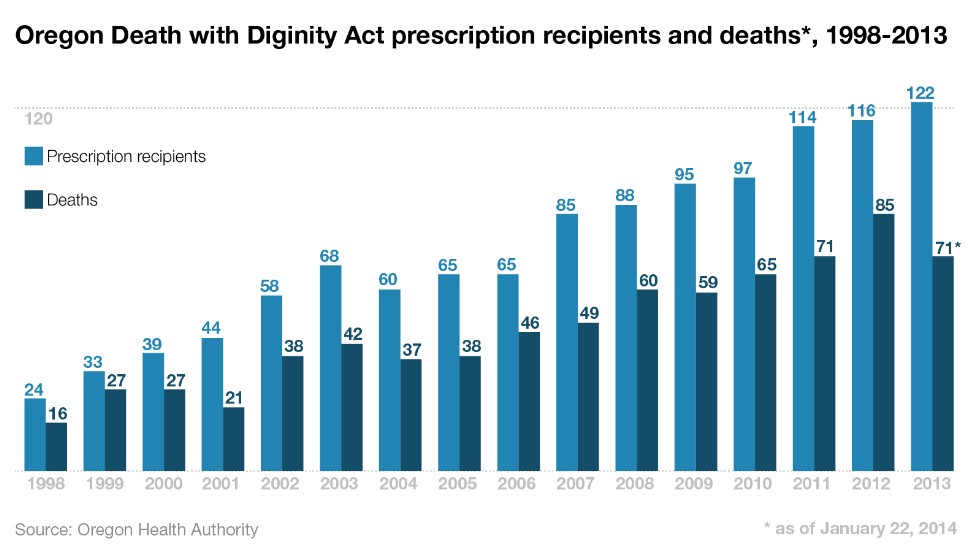
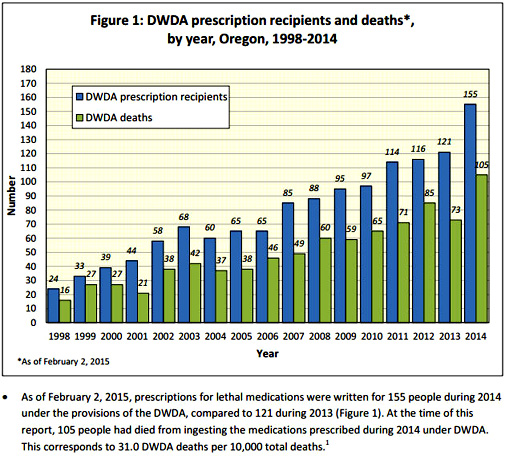
Oregon - Has had a physician-assisted suicide law on the books since 1997. Since its enactment, there has been a steady increase in both prescription recipients and the number of deaths. According to the 2015 evaluation report, since 1997, prescriptions have been written for 1,327 people and 859 patients have died from ingesting the drugs that were legally prescribed to them under the law.
Washington - According to the 2013 annual report, since 2009 prescriptions have been written for 549 people and there have been 525 reported deaths.
Vermont - Since May 2013, physician reporting forms have been completed for two people, according to the Department of Health.
Timeline:
June 1997 - The
U.S. Supreme Court rules that state laws banning physician-assisted suicide do
not violate the Constitution in the case Washington v. Glucksberg.
The court left the matter of the constitutionality of a right to a physician’s
aid in dying to the states.
October 27, 1997 - Oregon’s Death with Dignity Act becomes law. Passed in a 1994 election with 51% of voters in favor, the law was delayed initially because U.S. District Judge Michael Hogan issued an injunction and then ruled it unconstitutional. The Ninth Circuit Court of Appeals reversed the ruling and the injunction was lifted when the U.S. Supreme Court referred the matter back to the state in 1997.
November 1998 - American pathologist and assisted suicide advocate Jack Kevorkian, known as “Dr. Death,” videotapes the death of Thomas Youk, submits it to CBS’s 60 Minutes and it is broadcast on television. The airing prompts murder charges against Kevorkian, rather than assisted suicide charges, because Kevorkian injected the drug into Youk, who had Lou Gehrig’s disease.
March 26, 1999 - Kevorkian is convicted of second degree murder and delivery of a controlled substance. He serves eight years of a 10 to 25 year sentence.
November 4, 2008 - Washington’s initiative, the Death with Dignity Act, is passed with 57.91% of voters in favor.
March 5, 2009 - The Washington Death with Dignity Act goes into effect.
December 31, 2009 - A Montana Supreme Court ruling in the case Baxter v. Montana asserts that the Rights of the Terminally Ill Act protects a physician who prescribes aid from liability.
November 2012 - In Massachusetts, a death with dignity initiative appears on the November 2012 ballot. It is defeated by a slim margin with 51% voting against it.
May 20, 2013 - Vermont signs the Patient Choice and Control at End of Life Act into law.
January 13, 2014 - New Mexico Second Judicial District Judge Nan Nash rules in favor of an individual’s right to die in the case Morris v. Brandenberg. In appeal by the Office of the New Mexico Attorney General, the case is assigned to the New Mexico Court of Appeals/Supreme Court. The ruling remains in effect but only for Bernalillo County, according to the attorney general’s office.
November 1, 2014 - Brittany Maynard, a 29 year-old with terminal brain cancer, ends her life under Oregon’s “Death with Dignity Act.” She had moved to Oregon following her January 1, 2014 prognosis in order to take advantage of the Death with Dignity law. There is no such law in her native California. She garnered a large following advocating for physician-assisted suicide laws via social media.
October 5, 2015 - California governor, Jerry Brown signs into law the End of Life Option Act, which legalizes physician-assisted suicide for Californians with terminal illnesses. In a letter to members of the California State Assembly, Brown wrote that he thought about his own death while considering whether to sign the bill. “I do not know what I would do if I were dying in prolonged and excruciating pain. I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill.”
STATISTICS and DISCUSSION
Jul 13, 2014
40000
http://healthresearchfunding.org/physician-assisted-suicide-statistics/
Physician assisted suicide is a controversial, complicated matter that often polarizes the voting public. On the one hand, there are those who believe that patients suffering from chronic and fatal illnesses should be allowed to die with dignity, on their own terms and in peace. Having a doctor assist them with ending their own life allows them to stop this suffering and also ensures them that death will be on their own terms. No matter the side of the fence you sit when it comes to physician assisted suicide, you may be surprised to learn some statistics about this process and the legalities surrounding it, as well as public opinion and voter decisions in the past few years.
1. There is passive euthanasia and active euthanasia. Active euthanasia refers to ending a person’s life by active means, such as with drugs. This is typically what is meant by physician assisted suicide. Passive euthanasia refers to allowing a person to die by withholding drugs, food, water, and other substances needed for survival. This is not technically considered physician assisted suicide although there are legalities covering this process when a person relies on a physician for their health and life.
2. Some 9% of deaths in the Netherlands in 1990 were the result of physician-assisted suicide, as the practice is fully legal and commonly practiced. The practice is also legal for infants and newborns who are considered extremely disabled and has reportedly also been administered for those who were deemed “chronically depressed.”
3. In the Netherlands, it is reported that some 61% of those who received a lethal dose of painkillers did not know they were being euthanized, even though some 27% of those who received these doses were reported to be fully competent and able to make this decision.
4. It is also reported that some 10,000 citizens of the Netherlands carry a “Do Not Euthanize Me” card on their person at all times in case they are in an accident and unconscious or are taken to a hospital unexpectedly.
5. In the U.S., Oregon, Washington, and Montana have legalized the practice of physician assisted suicide, and in 2013, Vermont declared that suicide with prescribed medications was a legal “medical treatment.”
6. A report prepared by the U.S. Health Division stated that no patients who requested physician assisted suicide had uncontrolled pain. According to their reports, all patients who requested this procedure instead cited social and psychological concerns.
7. The Netherlands report a failure rate of physician assisted suicide at up to 25%, but the state of Oregon did not report any complications in a four-year period.
8. In the U.S., the Supreme Court ruled twice in 1997 that there is no constitutional precedent or right to assisted suicide.
9. The states of Alaska, Florida, and Hawaii have all voted down bills that would legalize physician assisted suicide, the state of Alaska declaring that there is no law in the state constitution that gives a person the right to this procedure. California, Washington, Maine and Michigan have consistently rejected physician assisted suicide issues for their ballots.
10. Texas law requires expectant mothers to be kept alive with no euthanasia practiced, even if brain dead and if previously stated wishes declared that no life support be administered, and regardless the term of her pregnancy.
11. In 2013, some 34% of Americans stated in a Pew Research poll that they had given serious consideration to their end of life decisions, up from 28% in 1990. Some 35% of those said that they had put their wishes in writing.
12. In the same poll, some 27% said that they had not given any thought as to their end of life decisions.
13. According to research, some 66% of U.S. adults believe that a doctor or nurse should allow a patient to die in certain circumstances.
14. Some 31% of U.S. adults surveyed believe that doctors and nurses should do whatever possible to save a patient’s life. In 1990, this number was only 15%.
15. A person’s ethnicity and race affect their views regarding end of life care. According to some research, 65% of white persons say they would cease all medical treatment if they suffered from an incurable disease or had chronic, debilitating pain. However, research shows that over 60% of blacks and some 55% of Hispanics would prefer their doctors to do everything possible to save their lives in the same circumstances. Religion News Service conducted interviews regarding these views and suggest the differences may be caused by religious faith and the roles of the family.
16. Views on assisted suicide are virtually equal when it comes to public opinion; the Pew Research found that 47% of Americans are in favor of passing physician assisted suicide laws for those that are terminally ill while a close 49% are opposed to these same laws.
17. This same research has shown that an American adult’s view regarding a person’s moral right to physician assisted suicide will vary based on the person’s individual circumstances.
18. While four states in the U.S. legally allow physician assisted suicide, only 673 patients chose to die with lethal injections prescribed by doctors from 1997 to 2012 in the state of Oregon. In the state of Washington, some 240 people chose physician assisted suicide from 2009 to the end of 2012. Some 100 other patients chose to end their life by taking advantage of the Death With Dignity Act but without medication. The state of Montana does not keep statistics on its citizens who choose physician assisted suicide. The state of Vermont has had only one citizen take advantage of their law, according to their reporting.
19. According to a brief submitted to a Canadian Special Senate Committee that was appointed to review Euthanasia and Assisted Suicide, cost control may become a factor in these cases.
20. This same brief noted that persons with disabilities and serious illnesses are often targets of violence more so than able-bodied persons, and that these crimes are often seen as being less serious and are treated as being less important by law enforcement. The brief noted that this devaluing of those with disabilities and illnesses has been carried over into the assisted suicide field, as happens in the Netherlands with disabled children and infants.
21. In 2006 a Gallup Poll asked if physicians should be allowed by legal means to end a person’s life using a painless procedure, if that person had a fatal disease that could not be cured and if that person and their family requested this procedure. Some 69% of those responding answered yes to the question.
22. The Hippocratic Oath, taken by those graduating medical school, originally prohibited against euthanasia along with abortion and surgery. The Oath, originally penned between 460 and 380 B.C., has since been revised.
23. The laws enacted in Washington and Oregon regarding physician assisted suicide do not require witnesses to be present when the lethal dose of medication is administered. Some have criticized this part of the law, stating that it may lead to abuses and especially elder abuse, or the administering of this procedure without a patient’s proper consent.
24. The Hemlock Society is one of the world’s largest and most active physician-assisted suicide support groups, and they openly state that they endorse this procedure for those who are not just terminally ill but for those who have “quality of life” issues. This would include those with illnesses that are not terminal and those who are disabled.
25. Dr. Jack Kevorkian spent eight years in prison for assisting in suicides before the procedure was legal. Dr. Kevorkian was a pathologist by trade, not a practicing doctor.
COMPLICATIONS
A debate in the American state of Iowa over the legalisation of assisted suicide prompted the Des Moines Register to survey how well in works.
In California, where it became legal on June 9, stories are already emerging that the letter of the law is not being observed. California multi-media and performance artist Betsy Davis died on July 23, one of the first to take advantage of the new law. She had ALS and since she was too weak to drink the lethal drugs herself, she was propped up by friends and someone, following instructions from a doctor, held the cup for her – which was probably illegal. The standard lethal drug, Seconal, was not available, so her friends mixed up a cocktail of drugs, hoping that they would work properly. She died four hours after swallowing the drugs, which is not the instant death that most people expect.
In Oregon where assisted suicide has been legal since 1998, and in Washington state, where it has been legal since 2009, the statistics from 1,642 deaths convey a mixed message.
Complications: about 2.5% experience complications, such as regurgitation, seizures, or waking up.
Incomplete records: in nearly 30% of cases, records are incomplete, even for important issues like complications.
Prolonged death: in Oregon the mean time before death was 25 minutes, but one person took four days.
No data: in Vermont and Montana, deaths are not tracked at all. There are no records. “Assisted suicide is nearly untraceable. There is minimal reporting and tracking,” Marilyn Golden, a senior policy analyst for the Disability Rights Education & Defense Fund in California, told The Register. “It almost appears as if the practice of assisted suicide has deliberately been made secretive, all with the claim of patient confidentiality.”
- See more at: http://www.bioedge.org/bioethics/behind-us-assisted-suicide-stats/12112#sthash.crMg9qLO.dpuf
California rolls back assisted suicide safeguards
By Jonah
McKeown
Sacramento,
Calif., Oct 7, 2021 / 15:10 pm
California Governor Gavin Newsom on Tuesday signed Senate Bill 380, a law that loosens several safeguarding requirements surrounding assisted suicide. The California Catholic Conference had been strongly urging opposition to the legal change.
“SB 380 does not offer genuine protection to patients and their families, nor does it ensure quality, equitable care for all,” the Catholic Conference wrote.
“We must protect vulnerable persons in times of weakness – the poor, elderly, people with disabilities, and others in vulnerable groups – from indifference, prejudice, abuse, exploitation, devaluation, and psychological and financial pressure to end their lives.”
Assisted suicide was legalized in California in 2015 by the End of Life Option Act, implemented under then-governor Jerry Brown. That act originally included a sunset clause and a legislative evaluation in 2026.
Existing California law required patients to make two separate requests, a minimum of 15 days apart, for assisted suicide medication. The law signed Oct. 5 shortens the required waiting period between the requests to 48 hours.
The new law also eliminates a requirement that the patient requesting assisted suicide make a “final attestation.”
The new law requires a healthcare provider who is unable or unwilling to participate in assisted suicide to inform the patient that they do not participate, document the date of the individual’s request and the provider’s notice of their objection, and transfer their relevant medical record upon request. Previously, healthcare providers who objected to assisted suicide were not required to refer patients to a provider who did not object.
“Stripping safeguards from the original assisted suicide law proves what opponents of assisted suicide laws have always claimed: That limitations on assisted suicide wouldn’t last for long once it was legalized,” Matt Vallière, executive director of Patients Rights Action Fund, an anti-assisted suicide organization, said Oct. 6.
“What California did yesterday lacked compassion and understanding. The effects of this law will be felt for years to come as people throughout the disability and aging community struggle to access quality healthcare.”
The conference noted that California’s assisted suicide law passed in the first place in part because of the safeguards and because of the sunset clause; the newly passed law extends the sunset clause to 2031.
There is “no data or science” to support the removal of such safeguards, the Orange County Register has noted. The Catholic conference has criticized the lack of data collected and a lack of transparency in the law’s implementation. Annual reports on the End of Life Option Act do not include any information on the reasons for patients requesting the lethal drugs.
The Catholic Medical Association, along with the U.S. Conference of Catholic Bishops and the Catholic Health Association, have repeatedly expressed support for palliative care as opposed to assisted suicide.
Palliative care involves medical care and pain management for the symptoms of those suffering from a serious illness, and refraining from taking actions that directly take the life of the patient, as opposed to the practices of assisted suicide and euthanasia.
In addition to California, assisted suicide is legal by law in Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia; and in Montana through a state supreme court ruling.
In 2018, Superior Judge Daniel Ottolia of Riverside County declared California’s assisted suicide law unconstitutional, ruling that the legislation was “adopted illegally” since it was passed during a legislative session limited to issues other than assisted suicide.
Then-California Attorney General Xavier Becerra— now U.S. secretary of health and human services— appealed Ottolia’s ruling in May 2018, and fought to reinstate the assisted suicide law.
The law was upheld by a January 2020 ruling of the Riverside County Superior Court, which determined that it was lawfully passed and did not violate the state constitution.
This Webpage was created for a workshop held at Saint Andrew's Abbey, Valyermo, California in 2014